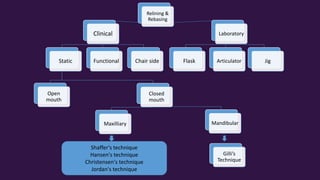
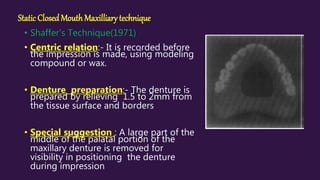
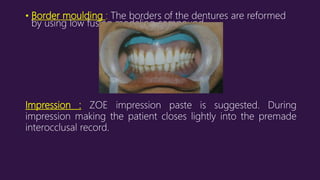
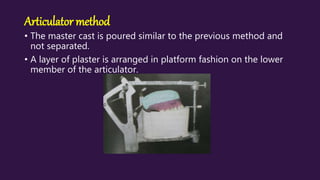
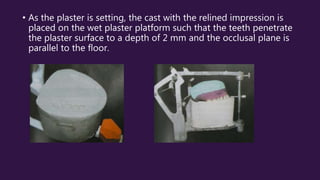
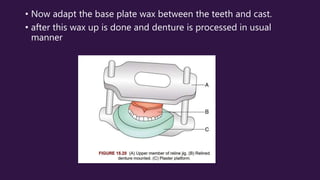
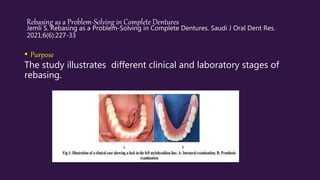
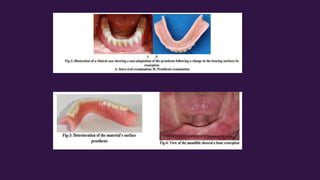
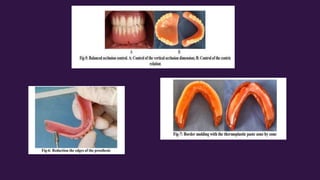
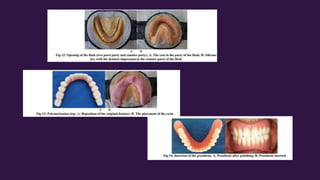
This document discusses relining and rebasing techniques for dentures. It begins with definitions, indicating that relining involves adding material to the denture base to improve fit, while rebasing replaces the entire denture base. It then covers indications, contraindications, tissue and denture preparation steps. Several static closed-mouth techniques for the maxilla and mandible are described, as well as open mouth and functional techniques. Finally, laboratory techniques like the flask, articulator and jig methods are summarized. The conclusion recommends regular recalls for relined or rebased dentures. A literature review covers a case report on a one-visit relining and a study evaluating resilient and hard denture liners.