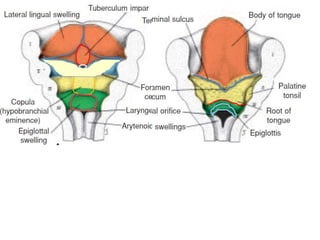
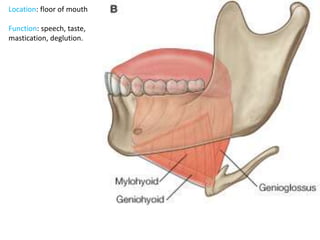
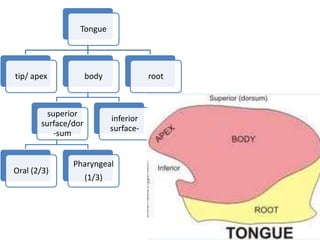
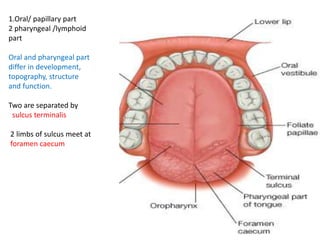
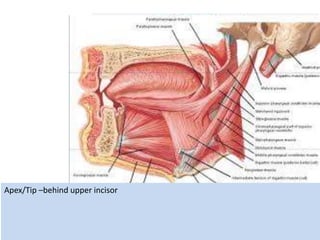
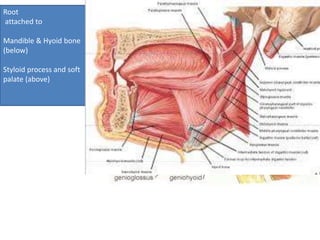
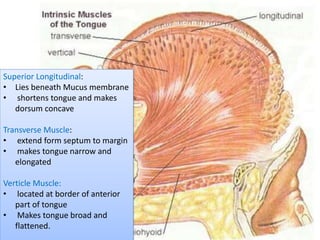
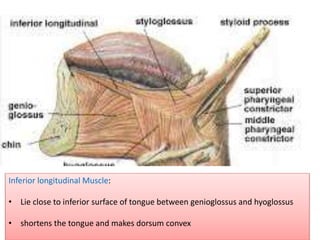
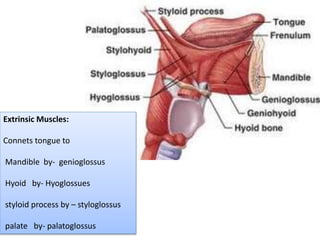
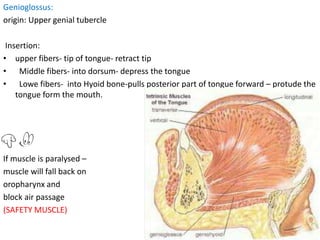
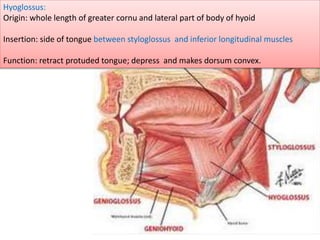
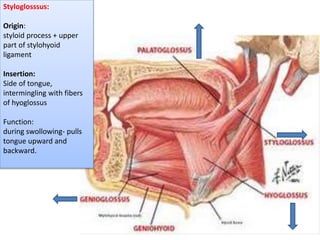
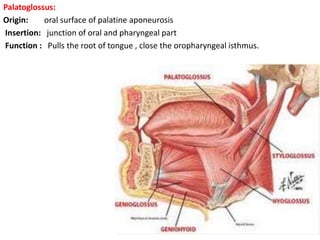
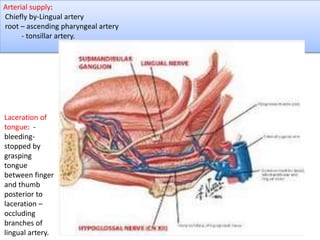
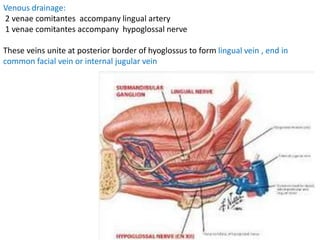


The tongue has oral and pharyngeal parts and is involved in speech, taste, chewing, and swallowing. It contains intrinsic and extrinsic muscles that alter its shape. The tongue has four types of papillae and receives its blood supply primarily from the lingual artery. Nerve supply involves the hypoglossal, lingual, and glossopharyngeal nerves. Injuries or conditions like glossitis can affect the structure and function of the tongue.























































































