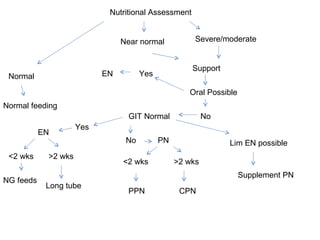
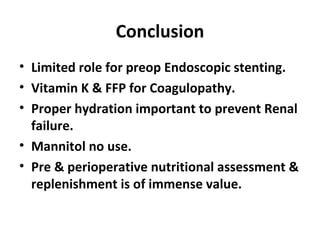
This document discusses various preoperative considerations for patients undergoing surgery, including endoscopic stenting, coagulopathy, hydration, nutrition, and nutritional assessment. It notes that endoscopic stenting preoperatively increases septic complications. For coagulopathy, it recommends vitamin K and fresh frozen plasma to improve coagulation factors. Proper hydration is important to prevent postoperative renal failure, though mannitol provides no benefits. Thorough preoperative and perioperative nutritional assessment and supplementation can be of great value for surgical patients.






























































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)




