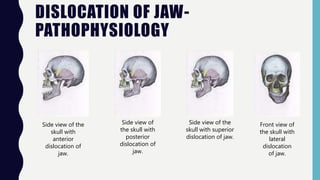
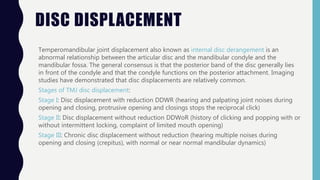
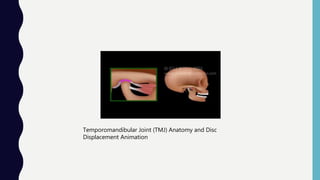
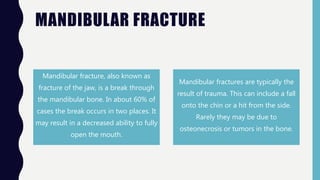
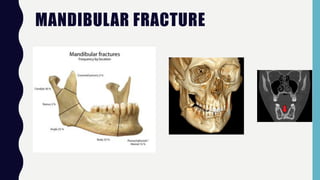
The temporomandibular joint (TMJ) connects the jawbone to the skull and allows for opening and closing of the mouth. It contains articular discs that divide the joint into compartments. TMJ disorders can cause pain, limited jaw movement, and joint noises. Common causes of pain include muscle issues, abnormal disc positioning, arthritis, and infections. Dislocated jaws may occur from trauma and cause difficulties opening the mouth. Displaced discs involve abnormal relationships between discs and bones. Mandibular fractures from falls or hits result in jaw pain and malocclusion.






![DISLOCATION OF JAW- SYMPTOMS
The symptoms can be numerous depending on the severity of the dislocation injury and how long the person is inflicted with the injury. Symptoms of a dislocated jaw include a
bite that feels “off” or abnormal, hard time talking or moving jaw, not able to close mouth completely, drooling due to not being able to shut mouth completely, teeth feel they are
out of alignment, and a pain that becomes unbearable
The immediate symptom can be a loud crunch noise occurring right up against the ear drum. This is instantly followed by excruciating pain, particularly in the side where the
dislocation occurred.[citation needed]
Short-term symptoms can range from mild to chronic headaches, muscle tension or pain in the face, jaw and neck.
Long-term symptoms can result in sleep deprivation, tiredness/lethargy, frustration, bursts of anger or short fuse, difficulty performing everyday tasks, depression, social issues
relating to difficulty talking, hearing sensitivity (particularly to high pitched sounds), tinnitus and pain when seated associated with posture while at a computer and reading books
from general pressure on the jaw and facial muscles when tilting head down or up. And possible causing subsequent facial asymmetry.
In contrast, symptoms of a fractured jaw include bleeding coming from the mouth, unable to open the mouth wide without pain, bruising and swelling of the face, difficulty eating
due to the constant pain, loss of feeling in the face (more specifically the lower lip) and lacks full range of motion of the jaw](https://image.slidesharecdn.com/prot-201119200454/85/TMJ-Temporomandibular-joint-17-320.jpg)













































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)
![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)










