
Recommended
More Related Content
What's hot
What's hot (20)
Similar to TMJ EVALUATION AND ITS ANATOMY.pptx
Similar to TMJ EVALUATION AND ITS ANATOMY.pptx (20)
Recently uploaded
Recently uploaded (20)
TMJ EVALUATION AND ITS ANATOMY.pptx
- 1. 7/3/2023 1 TMJ EVALUATION AND ITS ANATOMY Dr SIDHARTH R PILLAI Dr SIDHARTH RAVI PILLAI PG 1ST YEAR ORTHODONTICS AND DENTOFACIALORTHOPEDICS
- 2. 7/3/2023 2 CONTENTS • Introduction • Development of TMJ • Peculiarity of TMJ • General Anatomy of TMJ • Functional anatomy of TMJ • Mandibular movements and Muscle activity
- 3. 7/3/2023 3 • Examination & Diagnosis of TMJ Disorders • TMJ disorders • Treatment modalities • Recent Articles • Conclusion • References
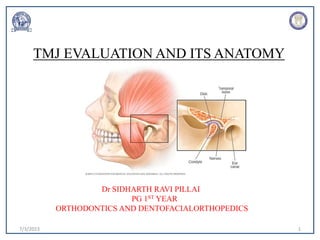
- 4. 7/3/2023 4 INTRODUCTION • The Temperomandibular Joint is formed by articulation between the Articular Eminence and the anterior part of the Glenoid Fossa of the squamous part of temporal bone above and the condylar head of the mandible below. • It’s a Synovial Joint of condylar variety.
- 5. 7/3/2023 5 • TMJ is considered as a Compound joint. • By definition, compound joint is articulation of atleast 3 bones yet the TMJ is made up of only Two bones. • But functionally, the articular disk serves as a non-ossified bone which permits the complex movements of the joint. • Thus the TMJ is considered as a compound joint.
- 6. 7/3/2023 6
- 7. 7/3/2023 7 PECULIARITY OF TMJ • Bilateral diarthrosis. • Articular surface covered by fibrous cartilage instead of hyaline cartilage. • Only bilateral joint that crosses the midline. • Only joint in the human body with rigid end point due to occlusion. • TMJ develops from distinct blastoma.
- 8. 7/3/2023 8 DEVELOPMENT OF TEMPOROMANDIBULAR JOINT • The early TMJ structures emerged progressively from a block of embryonic mesenchymal cells interposed between the developing temporal bone and mandible.
- 9. 7/3/2023 9 • This early block of mesenchymal tissue is a “developmental field” whose normal morphogenesis into discrete anatomic parts can be interfered with, in some significant and timely manner resulting in the anomalous development of one or more structures evolving from that “developmental field”
- 10. 7/3/2023 10
- 11. 7/3/2023 11 PRIMARY JOINT • At about 7th week of intrauterine life, the Meckel's cartilage extends from the midline backward and dorsally, acting as a scaffold to the developing mandible. • It terminates at the malleus and articulates with the incal cartilage forming the primary joint and any movement of the early jaws occur between them
- 12. 7/3/2023 12
- 13. 7/3/2023 13 SECONDARY JOINT • Two distinct regions of mesenchymal condensation (blastoma) appear at three months of gestation • Temporal Blastoma • Condylar Blastoma
- 14. 7/3/2023 14 TEMPORAL BLASTOMA • The first appearance of the temporal bone articular fossa occurs at 7 to 7.5 weeks. • The shape of the articular fossa is initially convex during the first weeks of its development up to 9 week. After that time, the fossa progressively takes on its definitive concave shape, which matches the shape of the condylar head.
- 15. 7/3/2023 15 . CONDYLAR BLASTOMA • The condensation and shaping of the mandibular condyle occur at about the same time as for the articular fossa. This mass is superiorly convex. • Condylar cartilage cells first appear between 9 and 10 weeks . The shape of this early cartilaginous condyle is that of the mesenchymal mass from which it arises.
- 16. 7/3/2023 16 • After the 10th week, the continuing ossification of the articular fossa appears more advanced in terms of increased cortical thickness and density of bony trabeculae.
- 17. 7/3/2023 17 The upper and lower joint cavities • They progressively appear as a group of small spaces or clefts. • mesenchymal tissue block that had earlier given rise to the articular fossa, disk, and condyle.
- 18. 7/3/2023 18 PARTS OF THE TMJ • Mandibular fossa • Condylar process • Joint capsule • Articular disc • Synovial fluid • Muscles and ligaments
- 19. 7/3/2023 19 MANDIBULAR FOSSA • Oval or oblong depression in the temporal bone just anterior to auditory canal.
- 20. 7/3/2023 20
- 21. 7/3/2023 21 CONDYLAR PROCESS • Convex on all bearing surfaces although somewhat flattened posteriorly • Its knob like form is wider latero-medially (20mm) than antero-posteriorly(8-10mm). • Its long axis is in a lateral plane. • Condyle is perpendicular to the ascending ramus of the mandible
- 22. 7/3/2023 22
- 23. 7/3/2023 23 JOINT CAPSULE • Temporomandibular joint is enclosed in a capsule that is attached at the borders of articulating surfaces of the mandibular fossa and eminence of the temporal bone and the neck of mandible. • The Capsule contains- • Internal Synovial layer • External fibrous layer containing veins, nerves and collagen fibers.
- 26. + 7/3/2023 26 • Articular disc is hypovascular, fibro-cartilaginous intra- articular sheet separating the condylar head from the glenoid fossa. • Divides the joint space into two compartments – the larger superior (1.2ml) and the smaller inferior (0.5ml) joint spaces. • Gliding movements and Hinge movements take place in the upper and lower compartments, respectively.
- 27. + 7/3/2023 27
- 28. + 7/3/2023 28
- 29. + 7/3/2023 29
- 30. 7/3/2023 30 SYNOVIAL FLUID • High amount of hyaluronic acid, giving it more viscosity. • The internal surface of the cavities are surrounded by specialized endothelial cells which forms a synovial lining. • This lining along with synovial fringe produces synovial fluid which fills both the joint cavities.
- 31. 7/3/2023 31 BOUNDARY LUBRICATION • It’s the primary mechanism of joint lubrication and prevents friction. • It occurs when the joint is moved and the synovial fluid is forced from one area of the cavity into another.
- 32. 7/3/2023 32 WEEPING LUBRICATION • It’s a secondary lubricating system and provides metabolic exchange. • Refers to the ability of the articular surfaces to absorb small amounts of synovial fluid. • During function, forces are created between articular surfaces which drive a small amount of synovial fluid in and out of the articular surfaces. Thus metabolic exchange occurs.
- 33. 7/3/2023 33 MUSCLES AND LIGAMENTS MUSCLES OF MASTICATION • Temporalis • Medial pterygoid • Lateral pterygoid • Masseter • Digastric
- 34. 7/3/2023 34 MASSETER • The masseter is a rectangular muscle that originates from the zygomatic arch and extends downward to the lateral aspect of the lower border of the ramus of the mandible. • Its insertion on the mandible extends from the region of the second molar at the inferior border posteriorly to include the angle.
- 35. 7/3/2023 35 • It has two portions, or heads: (1) The superficial portion consists of fibers that run downward and slightly backward, (2) The deep portion consists of fibers that run in a vertical direction.
- 36. 7/3/2023 36
- 37. 7/3/2023 37 TEMPORALIS • The temporalis is a large, fan-shaped muscle that originates from the temporal fossa and the lateral surface of the skull. • Its fibers come together as they extend downward between the zygomatic arch and the lateral surface of the skull to form a tendon that inserts on the coronoid process and anterior border of the ascending ramus. It can be divided into three distinct areas according to fiber direction and ultimate function.
- 38. 7/3/2023 38 • The anterior portion consists of fibers that are directed almost vertically. The middle portion contains fibers that run obliquely across the lateral aspect of the skull (slightly forward as they pass downward). • The posterior portion consists of fibers that are aligned almost horizontally, coming forward above the ear to join other temporalis fibers as they pass under the zygomatic arch.
- 39. 7/3/2023 39
- 40. 7/3/2023 40 MEDIAL PTERYGOID • The medial (internal) pterygoid originates from the pterygoid fossa and extends downward, backward, and outward to insert along the medial surface of the mandibular angle along with the masseter. • It forms a muscular sling that supports the mandible at the mandibular angle.
- 41. 7/3/2023 41 • When its fibers contract, the mandible is elevated and the teeth are brought into contact. This muscle is also active in protruding the mandible. • Unilateral contraction will bring about a mediotrusive movement of the mandible.
- 42. 7/3/2023 42
- 43. 7/3/2023 43 LATERAL PTERYGOID • For many years the lateral (external) pterygoid was described as having two distinct portions or bellies: an inferior and a superior. • Since the muscle appeared anatomically to be as one in structure and function, It is now appreciated that the two bellies of the lateral pterygoid function quite differently
- 44. 7/3/2023 44 The muscles will be described as Two Types- (1)The inferior lateral pterygoid (2) The superior lateral pterygoid.
- 45. 7/3/2023 45 INFERIOR LATERAL PTERYGOID • The inferior lateral pterygoid originates at the outer surface of the lateral pterygoid plate and extends backward, upward, and outward to its insertion primarily on the neck of the condyle.
- 46. 7/3/2023 46 SUPERIOR LATERAL PTERYGOID • The superior lateral pterygoid is considerably smaller than the inferior and originates at the infratemporal surface of the greater sphenoid wing, extending almost horizontally, backward, and outward to insert on the articular capsule, the disc, and the neck of the condyle.
- 47. 7/3/2023 47 DIGASTRIC MUSCLE • Although the digastric is not generally considered a muscle of mastication, it does have an important influence on the function of the mandible. • It has two bellies- Anterior belly and posterior belly
- 48. 7/3/2023 48
- 51. 7/3/2023 51 ARTICULAR LIGAMENTS • Ligaments are made up of collagenous connective tissues fibers that have particular lengths. • Three functional ligaments support the TMJ: (1) the collateral ligaments, (2) the capsular ligament, and (3) the temporomandibular ligament. There are also two accessory ligaments: (4) the sphenomandibular and (5) the stylomandibular.
- 52. 7/3/2023 52 COLLATERAL LIGAMENTS • The collateral ligaments attach the medial and lateral borders of the articular disc to the poles of the condyle. • The discal ligaments are true ligaments, composed of collagenous connective tissue fibers; therefore they do not stretch. • They function to restrict movement of the disc away from the condyle
- 53. 7/3/2023 53 Medial discal ligament • Attaches the medial edge of the disc to medial pole of condyle Lateral discal ligament • Attaches the lateral edge of disc to lateral pole of condyle.
- 54. 7/3/2023 54 ACTIONS: • Passive movement with the condyle • Hinging movement
- 55. 7/3/2023 55 CAPSULAR LIGAMENTS • The entire TMJ is surrounded and encompassed by the capsular ligament. • Superiorly Temporal bone along the borders of the articular surfaces of the mandibular fossa and articular eminence and inferiorly to the Neck of condyle.
- 56. 7/3/2023 56 • The capsular ligament acts to resist any medial, lateral, or inferior forces that tend to separate or dislocate the articular surfaces • A significant function of the capsular ligament is to encompass the joint, thus retaining the synovial fluid.
- 57. 7/3/2023 57 TEMPOROMANDIBULAR LIGAMENT • The lateral aspect of the capsular ligament is reinforced by strong, tight fibers that make up the lateral ligament or the temporomandibular ligament. • The Temporomandibular ligament is composed of two parts, an outer oblique portion and an inner horizontal portion
- 59. 7/3/2023 59 ACTION OF OUTER OBLIQUE • The oblique portion of the TM ligament resists excessive dropping of the condyle, therefore limiting the extent of mouth opening. • This portion of the ligament also influences the normal opening movement of the mandible
- 60. 7/3/2023 60 ACTION OF INNER HORIZONTAL • The inner horizontal portion of the Temporomandibular ligament limits posterior movement of the condyle and disc. • When force applied to the mandible displaces the condyle posteriorly, this portion of the ligament becomes tight and prevents the condyle from moving into the posterior region of the mandibular fossa.
- 61. 7/3/2023 61 CLINICAL IMPORTANCE • During trauma to the mandible ,effectiveness of this ligament demonstrated. • Neck of condyle will be seen to fracture before retrodiscal tissues are severed or condyle enters the middle cranial fossa.
- 62. 7/3/2023 62 SPHENOMANDIBULAR LIGMENT • Arises from spine of sphenoid bone and extends downwards to a bony prominence on medial surface of ramus called lingula. • Actions: no significant effect on limiting movements.
- 63. 7/3/2023 63 STYLOMANDIBULAR LIGMENT • The second accessory ligament is the stylomandibular ligament. • It arises from the styloid process and extends downward and forward to the angle of the posterior boarder to the Ramus of the Mandible. • The stylomandibular ligament therefore limits excessive protrusive movements of the mandible.
- 64. 7/3/2023 64 RELATIONS OF THE TMJ
- 65. 7/3/2023 65
- 66. 7/3/2023 66
- 67. 7/3/2023 67 TMJ INNERVATIONS Predominant vessels for TMJ are: • Superficial Temporal artery from the posterior • Middle Meningeal Artery from anterior • Internal Maxillary from Inferior alveolar artery
- 68. 7/3/2023 68
- 69. 7/3/2023 69 • Other important arteries are: Deep auricular, Anterior Tympanic and Ascending Pharyngeal arteries.
- 70. 7/3/2023 70 Nerve Supply: • Auriculotemporal nerve • Masseteric nerve • Deep temporal nerve
- 71. 7/3/2023 71 HISTOLOGY OF THE TMJ
- 72. 7/3/2023 72 HISTOLOGY OF ARTICULAR SURFACE • The Articular Surfaces of the madibular condyle and fossa are composed of four distinct layer. Articular Zone Proliferative Zone Fibrocartilaginous zone Calcified zone
- 73. 7/3/2023 73
- 74. Clear straw colored viscous fluid. Diffuses out from the rich capillary network of the synovial membrane. It contains: Hyaluronic acid-highly viscous May also contain some free cells mostly macrophages. 7/3/2023 74 HISTOLOGY OF SYNOVIAL FLUID • Clear straw colored viscous fluid. • Diffuses out from the rich capillary network of the synovial membrane. It contains: • Hyaluronic acid-highly viscous • May also contain some free cells mostly macrophages.
- 75. 7/3/2023 75 MANDIBULAR MOVEMENTS • Occurs as a complex series of inter-related 3D rotational and translational activities. • It is determined by combined and simultaneous activities of both TMJs. • Types of movements are - 1. Rotational movement 2. Translational movement
- 76. 7/3/2023 76 1. ROTATIONAL MOVEMENTS The process of turning around an axis ; movement of a body About its axis ,called the axis of rotation. In the TMJ, rotation occurs as movement within the inferior cavity of the joint. It is thus movement between the superior surface of the condyle and the inferior surface of the articular disc
- 77. 7/3/2023 77 HORIZONTALAXIS OF ROTATION • Mandibular movement around the horizontal axis is an opening and closing motion. • It is referred to as a hinge movement, and the horizontal axis around which it occurs is therefore referred to as the hinge axis
- 78. 7/3/2023 78 1.
- 79. 7/3/2023 79 VERTICALAXIS OF ROTATION • Mandibular movement around the frontal axis occurs when one condyle moves anteriorly out of the terminal hinge position with the vertical axis of the opposite condyle remaining in the terminal hinge position .
- 80. 7/3/2023 80
- 81. 7/3/2023 81 SAGITTAL AXIS OF ROTATION • Mandibular movement around the sagittal axis occurs when one condyle moves inferiorly while the other remains in the terminal hinge position
- 82. 7/3/2023 82
- 83. 7/3/2023 83 TRANSLATIONAL MOVEMENTS • In the masticatory system, it occurs when the mandible moves forward, as in protrusion. The teeth, condyles, and rami all move in the same direction and to the same degree
- 84. 7/3/2023 84
- 85. 7/3/2023 85 SINGLE PLANE BORDER MOVEMENTS • Mandibular movement is limited by the ligaments and the articular surfaces of the TMJs as well as by the morphology and alignment of the teeth. • When the mandible moves through the outer range of motion, reproducible limits result, which are called border movements result.
- 86. 7/3/2023 86 SAGITTAL PLANE BORDER AND FUNCTIONAL MOVEMENTS • Mandibular motion viewed in the sagittal plane can be seen to have four distinct movement components I. Posterior opening border II. Anterior opening border III. Superior contact border IV. Functional
- 87. 7/3/2023 87
- 88. 7/3/2023 88 POSTERIOR OPENING MOVEMENT • Posterior opening border movements in the sagittal plane occur as two-stage hinging movements.
- 89. 7/3/2023 89 ANTERIOR OPENING BORDER MOVEMENTS • With the mandible maximally opened, closure accompanied by contraction of the inferior lateral pterygoids (which keep the condyles positioned anteriorly) will generate the anterior closing border movement.
- 90. 7/3/2023 90
- 91. 7/3/2023 91 SUPERIOR CONTACT BORDER MOVEMENT • The superior contact border movement is determined by the characteristics of the occluding surfaces of the teeth. Throughout this entire movement, tooth contact is present. Its precise delineation depends on - • The amount of vertical and horizontal overlap of the anterior teeth, • The lingual morphology of the maxillary anterior teeth. • The general interarch relationships of the teeth.
- 92. 7/3/2023 92 FUNCTIONAL MOVEMENTS • Functional movements occur during functional activity of the mandible.. • They usually take place within the border movements and therefore are considered free movements. • Most functional activities require maximum intercuspation and therefore typically begin at and below the ICP.
- 93. 7/3/2023 93
- 94. 7/3/2023 94 HORIZONTAL PLANE BORDER AND FUNCTIONAL MOVEMENTS • When mandibular movements are viewed in the horizontal plane, a rhomboid-shaped pattern can be seen that has four distinct movement components and a functional component 1. Left lateral border 2. Continued left lateral border with protrusion 3. Right lateral border 4. Continued right lateral border with protrusion
- 95. 7/3/2023 95 LEFT LATERAL BORDER MOVEMENTS • With the condyles in the Centic relation position, contraction of the right inferior lateral pterygoid will cause the right condyle to move anteriorly and medially (also inferiorly). • If the left inferior lateral pterygoid stays relaxed, the left condyle will remain situated in CR and the result will be a left lateral border movement
- 96. 7/3/2023 96
- 97. 7/3/2023 97 CONTINUED LEFT BORDER WITH PROTRUSION • With the mandible in the left lateral border position, contraction of the left inferior lateral pterygoid muscle along with continued contraction of the right inferior lateral pterygoid muscle will cause the left condyle to move anteriorly and to the right
- 98. 7/3/2023 98
- 99. 7/3/2023 99 RIGHT LATERAL BORDER MOVEMENT • Contracting of the left inferior lateral pterygoid muscle will cause the left condyle to move anteriorly and medially (also inferiorly). • If the right inferior lateral pterygoid muscle stays relaxed, the right condyle will remain situated in the CR position. The resultant mandibular movement will be right lateral border
- 100. 7/3/2023 100
- 101. 7/3/2023 101 CONTINUED RIGHT LATERAL BORDER MOVEMENTS WITH PROTRUSION • With the mandible in the right lateral border position, contraction of the right inferior lateral pterygoid muscle along with continued contraction of the left inferior lateral pterygoid will cause the right condyle to move anteriorly and to the left.
- 102. 7/3/2023 102
- 103. 7/3/2023 103 FUNCTIONAL MOVEMENTS • As in the sagittal plane, functional movements in the horizontal plane most often occur near the ICP.
- 104. 7/3/2023 104 VERTICAL BORDER AND FUNCTIONAL MOVEMENTS When mandibular motion is viewed in the frontal plane, a shieldshaped pattern can be seen that has four distinct movement components along with the functional component: 1. Left lateral superior border 2. Left lateral opening border 3. Right lateral Superior Border 4. Right Lateral Opening Border
- 105. 7/3/2023 105 LEFT LATERAL SUPERIOR BORDER MOVEMENTS • With the mandible in maximum intercuspation, a lateral movement is made to the left. • The precise nature of this path is primarily determined by the morphology and interarch relationships of the maxillary and mandibular teeth that are in contact during this movement
- 106. 7/3/2023 106
- 107. 7/3/2023 107 LEFT LATERAL OPENING BORDER MOVEMENTS • From the maximum left lateral superior border position, an opening movement of the mandible produces a laterally convex path.
- 108. 7/3/2023 108
- 109. 7/3/2023 109 RIGHT LATERAL SUPERIOR BORDER MOVEMENTS • Once the left frontal border movements are recorded, the mandible is returned to maximum intercuspation. • From this position, a lateral movement is made to the right that is similar to the left lateral superior border movement.
- 110. 7/3/2023 110
- 111. 7/3/2023 111 RIGHT LATERAL OPENING BORDER MOVEMENTS • From the maximum right lateral border position, an opening movement of the mandible produces a laterally convex path similar to that of the left opening movement.
- 112. 7/3/2023 112
- 113. 7/3/2023 113 FUNCTIONAL MOVEMENTS IN FRONTAL PLANE • As in the other planes, functional movements begin and end at the ICP. • During chewing the mandible drops directly inferiorly until the desired opening is achieved. • It then shifts to the side on which bolus is placed and rises up.
- 114. 7/3/2023 114 • As it approaches maximum ICP, the bolus is broken down between the opposing teeth.
- 115. 7/3/2023 115 ENVELOPE OF THE MOTION • Superior surface is determined by tooth contacts, other borders are determined by ligaments and joint anatomy that restricts the movement. • It differs from person to person.
- 116. 7/3/2023 116 EXAMINATION AND DIAGNOSIS OF THE TMJ
- 117. 7/3/2023 117 HISTORY • History of onset, duration, frequency and dental treatment are important to assess the acute or chronic nature of the disease. • Factors like pain, click or dysfunction are to be considered while taking history.
- 118. 7/3/2023 118 CLINICAL EXAMINATION Inspection • Inter-incisal distance on mouth opening • facial asymmetry • deviation of mouth on opening and closing • preauricular swelling • Malocclusion or improper prosthesis, • Attrition of teeth decreasing vertical dimension should be noted.
- 119. 7/3/2023 119 DENTAL EXAMINATION • Any pre- mature contacts. • Evaluation for evidence of bruxism such as attrition of teeth, cheek or lip ridges caused by trapping of mucosa during clenching.
- 120. 7/3/2023 120 • Molar and canine relationship. • Freeway space, overjet, overbite, prosthesis. • Other oral habits and their possible effects on dentition, periodontium or other oral structures. • Number of missing teeth specially the posterior relationship which may predispose the TMJ to degenerative joint diseases.
- 121. 7/3/2023 121 RANGE OF MANDIBULAR MOVEMENT • Interincisal distance ranges between 35 to 50mm. • Lateral deviation of mandible in certain conditions are a significant sign. Abnormal protrusive movements are important and frequent, translation of condyles is the initial movement/sign. • Lateral motion should be 7 to 10mm in both sides • Normal protrusive range is between 7 to 10mm.
- 122. 7/3/2023 122 • Lateral aspect of TMJ is also palpated while opening and closing the mouth. • If the range of motion is limited attempt should be made to determine the cause: 1. Contracture of one or more muscle associated with jaw closure. 2. Non reducing anterior displacement of articular disc. (closed lock).
- 123. 7/3/2023 123 • Coronoid process interference. • Hematoma or infection. • Any other conditions such Fibrous ankylosis.
- 124. 7/3/2023 124 METHOD OF PALPATION
- 125. 7/3/2023 125 Palpation - • Tenderness on palpation suggests the presence of fracture, synovitis, or capsulitis of the joint. • Jaw is palpated for evidence of muscle enlargement and any unusual features such as movement of disc (hypermobility) during activity. • Overlying skin is checked for temperature and consistency in case of any inflammatory condition
- 126. 7/3/2023 126 Neurological test- • Trigeminal nerve supplies sensation to the superficial and deep structures of the head and face. • Sensory nerve activity is assessed by applying pressure , cotton wool and pin-pricks to the areas of distribution of trigeminal nerve. • This test helps in clinical diagnosis of myofascial pain.
- 127. 7/3/2023 127 Auscultation :- • Noise is assessed by stethoscope and classified either click (open or close click) or crepitus.
- 128. 7/3/2023 128 SPECIAL INVESTIGATIONS Laboratory investigation :- • Indicated when primary diseases are diagnosed by biochemical and serological tests. e.g. gout, infectious arthritis/ suppurative arthritis, rheumatoid arthritis. Electromyographic investigations :- • Helps in monitoring the activity of disordered TMJ
- 129. 7/3/2023 129 Drugs :- • Anti-inflammatory , muscle relaxants and antidepressants can be used to rule out the cause in myofascial dysfunction syndrome (MPDS).
- 130. 7/3/2023 130 Occlusal splints :- • To diagnose MPDS. Intermaxillary fixation :- • When there is pain of uncertain origin, IMF may be applied. • It is diagnostic as it relieves the pain if the source is the TMJ (condylar fracture) or masticatory muscles (prevents overstretching of muscles).
- 131. 7/3/2023 131 Local anesthesia :- To confirm the muscular pain. E.g. Injection in the masseter muscle
- 136. 7/3/2023 136 DISORDERS OF TMJ • The dental profession was first drawn into the area of Temporo- Mandibular Disorders by Dr. James Costen (1934) who described a group of symptoms that centered around the ear & TMJ.
- 137. 7/3/2023 137 • Refers to the group of disorders of the TMJ as a result of primary or secondary degenerative changes within the joint or muscle hyperfunction or parafunction.
- 138. 7/3/2023 138 CLASSIFICATION OF TMJ DISORDERS A. STRUCTURAL (DISORDERS ARISING WITHIN JOINT) 1.DEVELOPMENTAL I. Condylar hyperplasia II. Hemi mandibular elongation III.Hemi mandibular hyperplasia IV.Condylar hypoplasia and aplasia
- 139. 7/3/2023 139 2. ACQUIRED I. Traumatic arthritis II. Suppurative arthritis III.Osteoarthritis IV.Rheumatoid arthritis (RA) V. Psoriatic arthritis VI.Infection from disease that spreads from other tissue like TB , Syphilis
- 140. 7/3/2023 140 vii. Metabolic disorders like gout viii. Condylar fracture ix. Dislocation : acute , chronic, recurrent (habitual) x. Posttraumatic – ankylosis xi. Internal derangement xii. Tumors xiii. Synovial fistula and synovial cyst of TMJ xiv. Ankylosing spondylitis
- 141. 7/3/2023 141 B. FUNCTIONAL I. Disorders arising from structures outside the joint II. Myofascial pain dysfunction syndrome (MPDS)
- 142. 7/3/2023 142 CONDYLAR HYPERPLASIA • Condition of mandibular condyles creating overgrowth of the mandible, first described by Robert Adams.
- 143. 7/3/2023 143 Treatment :- • Condylectomy to ensure removal of the growing cartilage. • More conservative condylar shave (condyloplasty) can also be performed in certain cases. • Correction of facial asymmetry by orthognathic procedures or orthomorphic surgery.
- 144. 7/3/2023 144 HEMI MANDIBULAR ELONGATION • Horizontal displacement of the mandible and chin towards the unaffected side. • Lip line slopes towards the affected side.
- 145. 7/3/2023 145 • Lateral crossbite on the unaffected side. • In severe cases lateral open bite is observed on the affected side & in mild cases it is compensated by supraeruption of the teeth. • The displacement of the midline is greater at the anatomical mid-chin than at the incisor midline, so that there appears to be an apical drift of the incisors towards the unaffected side.
- 146. 7/3/2023 146 Treatment- • Condylar surgery is not necessary. • It is advisable to wait till the cessation of mandibular growth before jumping on surgical approach. • In addition genioplasty is sometimes necessary to achieve symmetry
- 147. 7/3/2023 147 HEMI MANDIBULAR HYPERPLASIA • This varies in the degree of development, depending on the age at which abnormal growth commences, the degree of abnormal growth and its duration. • It generally ceases after cessation of general growth but occasionally it continues for a few years.
- 148. 7/3/2023 148 • Inferior border lies at a lower level on the affected side. • No chin displacement but lip line slopes downwards to the affected side. • No midline shift with lateral open bite seen in some cases. • Downward cant of maxillary plane due to overeruption of teeth on the affected side. • Pain in the TMJ of the affected side.
- 149. 7/3/2023 149 TREATMENT During growth period , some form of condylar surgery (condylotomy, condyloplasty) will arrest and retard growth, thus limiting the secondary distortion. Treatment protocols are - • High condylectomy to arrest the growth. • Articular disc repositioning.
- 150. 7/3/2023 150 CONDYLAR HYPOPLASIAAND APLASIA • Characterized by facial deformity expressed on the affected side by a short mandibular ramus. • It can be Unilateral or Bilateral
- 151. 7/3/2023 151 UNILATERAL CONDYLAR HYPOPLASIA- • Shortening of mandibular vertical height occurs on the affected side. • A midline shift towards the same side. • Shifting of the chin towards the shorter side of the face. • Deviation of the mandible on mouth opening
- 152. 7/3/2023 152 • It can be congenital due to pharyngeal first and second arch malformation or it may result due to trauma ,infection or irradiation during growth period
- 153. 7/3/2023 153 Bilateral condylar hypoplasia - • Bilateral condition results in micrognathia or small mandible. • In congenital cases , it causes respiratory distress due to obstruction of pharyngeal airway by falling back of tongue.
- 154. 7/3/2023 154 Treatment :- • Severe mandibular dysostosis should be treated in growing age itself to produce to avoid secondary deformities because mandibular ramus is lengthened as the secondary dentition is erupting.
- 155. 7/3/2023 155 TRAUMATIC ARTHRITIS • Any traumatic incident involving the TMJ may lead to acute arthritis. • Site of inflammation is capsule. • Chronic trauma to the joint due to trauma from occlusion is also responsible for osteoarthrosis. • Characterised by, tenderness of the affected joint and restriction of the movement which cause mandible to swing on the affected side on opening.
- 156. 7/3/2023 156 • Oedema around the joint can be seen. • Pain in movement leads to classic trismus
- 157. 7/3/2023 157 Treatment :- • Treating the cause followed by physiotherapy. • Long term trismus may require surgical removal of coronoid processes and temporalis muscle attachment followed by physiotherapy.
- 158. 7/3/2023 158 OSTEOARTHRITIS • Most common skeletal disease of human body affecting the TMJ
- 159. 7/3/2023 159 • Earliest degenerative changes are seen in articular cartilage as preoteoglycans are lost at the surface. • Chondrocytes are stimulated and DNA synthesis increases. • Growth of surrounding bone is stimulated, resulting in osteophyte formation
- 160. 7/3/2023 160 • Pain in the joint and muscles of mastication, causing limitation of mandibular motion. • Joint noises, especially crepitus. • Osteophyte formation and marginal bone thickening leads to palpable masses over preauricular region.
- 161. 7/3/2023 161 Treatment :- • Initial intervention should limit excessive and recurrent trauma. • Moderate exercise and physical therapy should be started to strengthen the musculature supporting the joints. • NSAIDs to reduce pain. • In severe case, thermal therapy can be obtained with ultrasonography and infrared heat.
- 162. 7/3/2023 162 RHEUMATOID ARTHRITIS • Autoimmune disease commonly affecting diarthrodial joints. • It can affect the joint at any age. • Juvenile rheumatoid arthritis (Still's disease) may be of varying severity
- 163. 7/3/2023 163 Pathophysiology :- • Synovial membrane proliferation and outgrowth causes erosion of articular cartilage and subchondral bone. • The production of inflammatory mediators, which is stimulated by the cells, result in the production of proteinases and prostaglandin. Collagenases are responsible for typical erosions seen over the joint surface
- 164. 7/3/2023 164 Clinical Feature- • Clicking, crepitus and tenderness of the joint on palpation. • Limitation of motion occurs as the bone is destroyed and joint space is filled with scar tissue leading to fibrous ankylosis. • Progressive class II occlusion develops resulting in retrognathia,bird-face deformity and apertognathia may result in young children.
- 165. 7/3/2023 165 TREATMENT- • Anti inflammatory drugs (salicylates, NSAIDs, corticosteroids), soft diet, avoiding extreme jaw movements. • If NSAIDs are ineffective, disease modifying anti-rheumatic drugs like hydroxychloroquine, penicillamine .
- 166. 7/3/2023 166 PSORIATIC ARTHRITIS • Resembles the rheumatoid type, but it is associated with psoriasis, a dermatologic disease. • remission of joint disturbances coincident with the skin lesions differentiate the disease from rheumatoid arthritis. • There is a high incidence in women
- 167. 7/3/2023 167 Clinical features :- • TMJ involvement is described as episodic, sudden and usually unilateral. • Limitation of mandibular movements. • Morning stiffness, crepitus, eventual loss of interincisal opening. • In advanced disease, ankylosis can occur.
- 168. 7/3/2023 168 Treatment- • Systemic treatment should be undertaken. • Reduce loading on the joint. • In severe cases, immunosuppressive agents such as methotrexate have been used.
- 169. 7/3/2023 169 TUMOURS • Any tumour in the area of TMJ and/or muscles of mastication can significantly cause jaw hypomobility. • Both benign and malignant lesions affect the condyles and synovial components of the joint.
- 170. 7/3/2023 170 ANKYLOSING SPONDYLITIS (Marie- Strumpell disease) • Chronic inflammatory disease involving the articulators of spine adjacent soft tissues. • High sex ratio of male:female (8:1)
- 171. 7/3/2023 171
- 172. 7/3/2023 172 Clinical features :- • Symptoms are due to imperfect head posture caused by the vertebral lesions. • The most common complaints are of pain, stiffness, decreased range of motion and eventually ankylosis. • Extra-articular manifestations such as cardiac symptoms are common in patients with TMJ involvement
- 173. 7/3/2023 173 Treatment :- • The load must be reduced across the joint by the use of acrylic splints. • The drug with proven efficacy sulphasalazine. • Surgical intervention should be limited to those patients with severe crippling disease.
- 174. 7/3/2023 174 DISORDERS ARISING FROM OUTSIDE THE JOINT • The most common disorders outside the joints that cause pain around the joints are • Fibromyalgia • Polymyalgia rheumatica • Bursitis or tendinitis • Bursitis and tendinitis often result from injury, usually affecting only one joint. However, certain disorders cause bursitis or tendinitis in many joints.
- 175. 7/3/2023 175 MYOFASCIAL PAIN DYSFUNCTION SYNDROME (MPDS) • This condition is the most common disorder affecting the temporomandibular region. It is more common among women . • In the affected muscle, both pain and trigger points (which cause referred pain) may result from parafunctional behavior such as bruxism (clenching or grinding of the teeth), which is regarded as two distinct entities: sleep or awake bruxism, which have different etiologies.
- 176. 7/3/2023 176
- 177. 7/3/2023 177 • Symptoms include pain and tenderness of the masticatory muscles and often pain and limitation of jaw excursion. • Both sleep bruxism and sleep- disordered breathing (such as obstructive sleep apnea and upper airway resistance syndrome) are associated with headache that is more severe on awakening and gradually subsides during the day.
- 178. 7/3/2023 178 • The jaw deviates when the mouth opens but usually not as suddenly or always at the same point of opening as it does with internal temporomandibular joint derangement
- 179. 7/3/2023 179 DIAGNOSIS • Clinical evaluation • Sometimes polysomnography • A simple test may aid the diagnosis: 2 or 3 tongue blades are placed between the rearmost molars on each side, and the patient is asked to close the mouth gently • The distraction produced in the joint space may ease the symptoms.
- 180. 7/3/2023 180 • X-rays usually do not help, except to rule out arthritis. • If giant cell arteritis is suspected, erythrocyte sedimentation rate (ESR) is measured. • Polysomnography should be done if sleep-disordered breathing is suspected.
- 181. 7/3/2023 181 Treatment • Mild analgesics • Oral appliances • Possibly temporary use of an anxiolytic or cyclobenzaprine at bedtime • Trigger point injections and other physical and behavioral therapy modalities
- 182. 7/3/2023 182 ORTHODONTIC TREATMENT AND TMJ Twin block therapy- • There was a significant change in the condylar dimensions: • Increase in length, width, and height by 1.28, 0.88, 1.59 on the right and by 1.60, 0.53, and 1.10 mm on the left sides, respectively. • There was significant forward positioning of the right and left condyle by 1.5 and 1.3 mm, respectively. Younes Elfeky et al 4 (2018). Three-dimensional skeletal, dentoalveolar and temporomandibular joint changes produced by Twin Block functional appliance. Journal of Orofacial Orthopedics / Fortschritte der Kieferorthopädie. 10.1007/s00056-018-0137-1
- 183. 7/3/2023 183 Condylar position and joint spaces after maxillary first premolar extraction in skeletal Class II malocclusion :- • There was a statistically significant (P≤.05) posterior positioning of the condyle relative to the vertical plane. • The distance increased significantly from 5.77 to 6.82 mm as this plane is anterior to the mandibular condyle. Alhammadi MS, Fayed MS, Labib A. Three-dimensional assessment of condylar position and joint spaces after maxillary first premolar extraction in skeletal Class II malocclusion. Orthod Craniofac Res. 2017 May;20(2):71-78. doi:10.1111/ocr.12141.Epub 2017 Feb 1. PubMed PMID: 28150380.
- 184. 7/3/2023 184 • There was an increased anterior joint space (from 3.10 to 3.90 mm) and decreased posterior joint space (from 2.78 to 2.23 mm) following treatment. • No changes were observed in mediolateral and vertical condylar positions.
- 185. 7/3/2023 185 CONCLUSION • As dental practitioners, we seldom examine the TMJ during routine examination. Though treating the cause is important, it’s also duty of a dentist to thoroughly examine the patient, identify any underlying asymptomatic disorders, and educate and motivate the patient to take up preventive measures & early treatment to avoid further symptoms that serve as precursors to TMJ disorders.
- 186. 7/3/2023 186 REFERENCES • Management of Temporomandibular Disorders & occlusion- Jeffrey p. Okeson • White and Pharoah book of Oral radiology • Human anatomy 3rd Volume; 3rd edition - B.D.Chaurasia • Color atlas of dental medicine- tmj disorders and orofacial pain- alex bumann, ulrich lotzmann • Human Embryology 8th Edition – Inderbir Singh • Textbook of Human Histology with Colour Atlas 5th edition - Inderbir Singh
- 187. 7/3/2023 187 REFERENCES • Wheeler's Dental Anatomy, Physiology and Occlusion 9th edition - Nelson fausto • Orbans Oral Histology & Embryology 13th edition – G S kumar • Younes Elfeky, Hanem & Fayed, Mona & Alhammadi, Maged & Abou Zeid Soliman, Sanaa & Mohamed El Boghdadi, Dalia. (2018). Three-dimensional skeletal, dentoalveolar and temporomandibular joint changes produced by Twin Block functional appliance. Journal of Orofacial Orthopedics / Fortschritte der Kieferorthopädie. 10.1007/s00056-018-0137-1.
- 188. 7/3/2023 188 REFERENCES • Alhammadi MS, Fayed MS, Labib A. Three-dimensional assessment of condylar position and joint spaces after maxillary first premolar extraction in skeletal Class II malocclusion. Orthod Craniofac Res. 2017 May;20(2):71-78. doi:10.1111/ocr.12141.Epub 2017 Feb 1. PubMed PMID: 28150380.
Editor's Notes
- The area where the mandible articulates with the temporal bone of the cranium is called the TMJ.
- The embryonic development of the temporomandibular joint differs considerably from that of other synovial joints. Most synovial joints complete the development of their initial cavity by the 7th week post conception, but the temporomandibular joint does not start to appear until this time.
- The critical period in the early prenatal morphogenesis of the human temporomandibular joint during the time of early 7 to 11 weeks of fertilization age
- he chronological events leading to development of the temporomandibular joint
- This is meckel cartilge goes backward and articulate with the incal cartigae
- Temporal blastoma gives rise to articular eminence and glenoid fossa Spicules of primary cancellous bone appear at 10 to 11 weeks
- These small spaces or clefts between the mesenchymal cells in the area gradually enlarge and combine into larger spaces or cavities superior and inferior to the disk
- Intra –articular disc
- It is biconcaveThe condyle is normally situated on the thinner intermediate zone (IZ) of the disc. • The anterior border of the disc (AB) is considerably thicker than the intermediate zone, and the posterior border (PB) is even thicker
- it can be roughly divided into anterior band (2mm thick), posterior band (3mm thick), an intermediate band (1mm thick) and a bilaminar or retrodiscal region most posteriorly.
- Divides the joint space into two compartments – the larger superior (1.2ml) and the smaller inferior 0.5ml
- IT HAS TWO PURPOSE THAT IS METABOLIC AND LUBRICANT..it consist small cell called synoviocytes
- When joint moves sf forced from one area of cavity into anthr and it prvnt friction durng action
- All the muscles dev from the mesenchyme of the 1st brachial arch
- Arise from the za insert into lateral border of r of mndible
- Sp goes downward slight obliquly where dp goes down straight
- Arises from the temporal fossa from lateral part of skull goes downward inserted into coronoid p
- It can be divided into three distinct areas according to fiber direction and ultimate function.
- Arises from pterygoid fosa and goes downward inserted into angle of mand
- Arises frm lateral ptrygd and insert into condyle
- Arises from infratempl region backrd and downwrd to articular cap
- A b orginates from Lin.csurface of mand and insert into intermdte tendon p. B aries from mastd notch insert to hyoid bone
- A b orginates from Lin.csurface of mand and insert into intermdte tendon p. B aries from mastd notch insert to hyoid bone
- Ligaments do not enter actively into joint function but instead act as passive restraining devices to limit and restrict border movements
- Cmly called the disscal ligaments -2 types medial disc l lateral discal lig
- It helps in retaing the fluid Also prvd proprioceptive feedback regrd pos. and mov.
- The TM ligament therefore protects the retrodiscal tissues from trauma Protects the lateral pterygoid muscle from extension
- Anatomic structre are
- Tmj is suppld from vrty of vessels condyle receives vasculr supply
- Condyle receives its vascular supply through its marrow spaces by way of Inferior Alveolar Artery
- Most innrvt prvds by auriculotmp nerve and also trigml nerve
- A- clgn fib at centr b – irrg clge fibre c. large marrow space d articulr srf and mand fosa
- AZ is made up of dense fibrous cnnt tissue rather than hyline .superfacial lyr PZ-this lyr resble for prolifrtn of articular cartige undifrnt mesenchyml tissue FC- PRVD 3 D netrk agnst com and lat force Cz- deepst zone in this ther prs of chndrblast cell
- R m occur in thre plane horizontal ,vertical,sagital
- Mand mv arnd the horizontl axis is an opng and closg .pure rotatiob movmt does not accpd by transltnl movmt
- Movmt occurs when one condyle moves ant while other at terminal hng pos
- Movmt around the sagitl axis one condyle moves inferiorly while other at terminal hinge position.
- Movg object has same velocity and direction.
- The range of posterior and anterr openg border movemt is determd or limited primarly by lig and morphly of tmj
- The condyle are stblizd in the most super position from which hinge axis occr in centric rltn
- Cndyle stbld in antr postn a pure hinge axis occur as mand closg from maximim protrv postn
- his border movement is solely tooth determined, changes in the teeth will result in changes in the nature of the border movement
- When the mandible is at rest, it is found to be located approximately 2 to 4 mm below the ICP
- The mand is posturl positn PP located same 2 to 4 mm below intra cuspal pos
- contraction of the right inferior lateral pterygoid will cause the right condyle to move anteriorly and medially
- Since the right condyle is already in its maximum anterior position, the movement of the left condyle to its maximum anterior position will cause a shift in the mandibular midline back to coincide with the midline of the face
- Contracting of the left inferior lateral pterygoid muscle will cause the left condyle to move anteriorly and medially (also inferiorly).
- contraction of the left inferior lateral pterygoid will cause the right condyle to move anteriorly and to the left.
- During chewing the range of jaw movement begins some distance from the maximum ICP; but as the food is broken down into smaller particle sizes, jaw action moves closer and closer to the ICP.
- s
- secondary influence are the condyle-disc-fossa relationships and mrphlogy of the wrkig or rotating side TMJ. The maximum lateral extent of this movement is determined by the ligaments of the rotating joint
- As maximum opening is approached, ligaments tighten and produce a medially directed movement that causes a shift back in the mandibular midline to with the midline of the face
- Once the left frontal border movements are recorded, the mandible is returned to maximum intercuspation.
- As maximum opening is approached, ligaments tighten and produce a medially directed movement that causes a shift back in the mandibular midline to coincide with the midline of the face to end this left opening movement
- In the final mm of closure the mandible quickly shifts back to the ICP.
- By combining mandibular movements in all three planes, a 3D envelope of motion can be produced that represents the maximum range of movement of mandible
- History of trauma and history of dental treatment can usually pinpoint the etiology of the disease.
- Palpate directly over the joint while the patient opens and closes the mandible, and the extent of mandibular condylar movement can be assessed
- The normal joint functions relatively quietly. crepitus or grinding and clicking or popping sounds rules out prnse abnormlty in tmj
- If pain subside its indicate presence of underlyng cause of the pain in muscle
- OPG is a panoramic or wide view x-ray of the lower face, which displays all the teeth of the upper and lower jaw on a single film.
- the x-ray beam is directed parallel to the long axis of the condyle. At this angulation, the cranial bones are the only structures superimposed over the joint.
- IT PRVDE SAGITAL VIEW OF THE MEDIAL CONDYLE
- transmaxillary projection shows the oblique frontal aspect of the condyle and articular eminence
- Difficulty in Deglutation and swallowing. Pain can aggregate while opening of the jaw. Difficulty in Breathing while sleeping. Difficulty in speech and other oral function
- Mild mandibular protrusion
- Always presents with the same general appearance as hemi mandibular elongation.
- Bird like face, retruded chin with a small mandibular arch.
- Tretm can also achievd by graft ,distrction osteogensis,grft ,surgey
- Chrnc noninflmty and degentv disese affting articlr surface of joint
- After microvascular injury, synovial cells proliferate, swell and are infiltrated by mononuclear cells and T lymphocytes