2. INTRODUCTION
• TMJ – Complex joints of the body.
• Area where mandible articulates with the cranium.
• GINGLYMOARTHROIDAL JOINT
Ginglymoid – Hinging
Arthroidal – Gliding
• COMPOUND JOINT
• SYNOVIAL JOINT of the condylar variety
3. Unique features
• Bilateral diarthrosis - right and left sides function
together.
• Articulation surface covered by fibro cartilage instead
of hyaline cartilage.
• Because fibrous connective tissue is generally less
susceptible than hyaline cartilage effects of aging, is
less likely to break down over time.
• better ability to repair than does hyaline cartilage.
• In contrast to other diarthrodial joints TMJ is last joint
to start developing about 7th week in utero.
4. DEVELOPMENT OF TMJ
• The critical time area in the formation of the human
temporomandibular joint is from the eighth to the tenth weeks
of fetal life.
• During this period proliferation and histodifferentiation of the
embryonic mesenchyme take place and the condyle of the
mandible assumes its mature morphologic pattern.
5. MORPHOGENESIS
• 2 sets of articulation are present – primary and secondary
• Condylar cartilage and muscle fibres have important role in
development of the joint
6. • Morphogenesis – critical period of about 7-11 weeks of
gestation
• 10 – 11 weeks – Ossification of the temporal components
occurs
• 12 weeks – Condylar cartilage becomes conspicuous
– Mesenchyme condenses to form the articular
disc
• 13 weeks – Joint cavities formed
• 14 weeks – Joint development completed
7. • Condylar cartilage
20th week – Endochondral ossification except head of
condyle which remains as cartilage
• Fossa
9th week – Shape of fossa
22nd week – Fossa can be distinguished
Articular eminence becomes evident
• Disc
19-20 wks – Disc takes on its fibrocartilage tissue
composition
8. • Capsule
26 weeks – Definite cellular morphology of capsule and
synovial lining
• Joint cavity
14 weeks – Both cavities are evident
9. TMJ inthefirstdecadeoflife
• During the first year of life the condyle : vascularization, entire
cartilage layer becomes significantly thinner. This continues upto
the third year.
• Morphologic changes take place from birth to the end of mixed
dentition period: Enlargement of articular eminence and post
glenoid region.
• During this time tympano-squamosal tissue begins to close
as the postglenoid process becomes fused with the
tympanic plate.
• By 2 ½ years the articular eminence increase from 2 to
4mm.
10. • This is due to resorption of the bone in the roof of the
mandibular fossa and bone deposition anterior and
posterior to the fossa leading to formation of ‘S’ shape
curve.
• The process continues so that by 6-7 years the articular
eminence enlarges to 5-6mm in height.
11. By approximately 6-7 years of age ;
• Articular layer of condyle becomes thicker
• Cartilage layer becomes thinner – 0.3mm
• Underlying trabeculae becomes progressively thicker.
• Growth continues - 7 to 12 years of age.
• Articular disk – highly vascularized and rich in
fibroblasts during the 1st few years.
12. • Progressively the vascularization decreases.
• Posterior surface of the ramus, the condylar neck and
the condyle are sites of active skeletal growth leading
to relocation of the mandibular condyle in superior and
posterior direction (V principle of Enlow)
13. TMJ in2ndand3rddecade:
• Characterized by progressive slowing of growth process.
• By 13-15 years decreased thickness of cartilage layer.
• Presence of proliferative layer atleast till age of 18 years.
• A cortical bone cap coalescing with subchondral
trabecular bone by 10-12 years of age. This increases in
thickness upto 3rd decade of life.
• Bone cap is completed by 20 years of age although
cartilage and sparse cartilage cells remain.
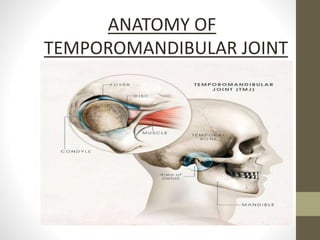
14. Components of the joint
It is an articulation between the squamous portion of the
temporal bone and the mandible.
16. MANDIBULAR FOSSA
• Also called as Mandibular fossa
• Concave depression in inferior surface
of petrous temporal bone
• Boundaries:
Posteriorly – Petrotympanic fissure
Anteriorly – Articular eminence
• Covered by a thin fibrous layer
• Roof of fossa – thin & separates the brain from the joint cavity
• Care – avoid perforation
17. ARTICULAR EMINENCE
• Present anterior – Glenoid fossa
• Consists of
1. A descending slope
2. A transverse ridge
3. An ascending slope
• Covered by dense , compact fibrous
tissue – collagen
• Thickest – descending slope
• Subjected to loading during function
18. CONDYLE
• Elliptical in shape
• Long axis is 90 degree to body of
mandible
• Mediolateral width( 18-23 mm)
Anteroposterior width (8-10 mm)
• Has lateral & medial tubercles, provide
attachments to lateral & medial collateral
ligaments.
19. ARTICULAR DISC
• Fibrocartilage made up primarily of dense collagen &
occupies space between condyle & mandibular fossa
• Avascular
20. • Upper surface – concavoconvex
• Under surface - concave
• Divided into 3 regions
An anterior fibrous band ( ant disc ligament)
Central area thinnest – Intermediate zone
Posterior fibrous band ( post disc ligament)
• Anterior & posterior borders - thicker
21. • Disc is also attached to the condyle medially and laterally by the collateral
ligaments.
• Divides the joint – distinct cavities
Upper / superior cavity- bordered – mandibular fossa & superior surface
of disc
Lower / inferior cavity – mandibular condyle & inferior surface disc
22. • Synovial fluid fills cavity
• Volume of upper cavity – 1.2ml & lower cavity – 0.9ml
• Retrodiscal tissue is present.
• Bilaminar zone
Superior retrodiscal lamina( SRL) – elastic fibers
Inferior retrodiscal lamina(IRL) – collagen fibers
23. • Functions of articular disc
i. Helps stabilize tmj.
ii. Acts as a shock absorber.
iii. Shape and thickness - governed by muscle forces controlling position
of mandible and condyle
iv. reduces frictional wear – spread of lubrication
24. SYNOVIAL MEMBRANE
• Two in number – placed one above, and the other below, the
articular disc
• Lines the inner surface of the capsule - relatively delicate.
• Finger like projections – villi – seen in anterior and posterior limits
of the joint
26. SYNOVIAL FLUID
• Internal cavities surrounded by specialised endothelial cells form
synovial lining produces synovial fluid.
• Fills the joint cavities
• Functions
1. Lubricant reduces friction
2. Medium for metabolic requirements
Lubrication – two mechanisms
• Boundary lubrication
• Weeping lubrication
27. LIGAMENTS
• Act as passive restraining devices to limit & restrict border movements.
• Three Functional ligaments
1. Collateral ligament
2. Capsular ligament GRAYS FIG 8.129
3 .Temporomandibular ligament
• Two Accessory ligaments
1. Sphenomandibular ligament
2. Stylomandibular ligament
28. Collateral ligament
• Attach the medial & lateral borders of the articular disc to the
poles of the condyle
• Also called as discal ligament
• Two in no
Medial Lateral
• Responsible for dividing the joint mediolaterally into superior &
inferior joint cavities.
29. Functions
1. Restricts movement of the disc away from the condyle.
2. Allows the disc to move passively with the condyle as it glides
anteriorly & posteriorly.
3. Responsible for the hinging movements of the TMJ.
30. Capsular ligament
• Surrounds & encompasses the entire TMJ
• Attachments
Superiorly – temporal bone,
mandibular fossa & articular
eminence
Inferiorly – neck of the condyle
• Well innervated
Capsular ligament
31. Functions:
1. Acts to resist forces that tend to seperate or dislocate the articular
surfaces.
2. Provides propioceptive feedback
33. Sphenomandibular ligament
• Remnant of Meckel’s cartilage
• Functions
(i) Primary passive support
of mandible
(ii) Serves as a fulcrum
(iii) Protects the blood vessels
and nerves during
movements (Moss, 1959)
34. Stylomandibular ligament
• Thickened band of the
cervical fascia
• Ligament is loose when mouth
is closed and wide open;
tense when maximally
protruded
• Functions
(i) Does not contribute significantly to the
strength of the joint
(ii) Limits excessive protrusive movements
35. Nerve supply
• Sensory innervations
– auriculotemporal n.
• Proprioception
– deep temporal n.
– masseteric n.
39. BIOMECHANICS OF THE JOINT
• TMJ is a compound joint
• Its structure & function can be divided into 2 distinct systems
• One joint system
• Inferior synovial cavity
• Condyle disc complex
• Rotational movements of tmj
40. • Second joint system
• Condyle disc complex functioning against the surface of the mandibular
fossa
• Translation movement of tmj
41. Movements of the TMJ
Movements of the TMJ are chiefly by the muscles of mastication.
42. Closed mouth position
• Condyle rests in the thinnest part, the intermediate zone,
against the posterior slope of the articular eminence
• The thick posterior band of the disc lies immediately above the
condyle
43. Opening of the mouth
• Two distinct motions :
• First 20 mm – rotation – limited opening
• Intermediate zone becomes the articulating surface
Inferior head of lateral pterygoid contracts
Superior retrodiscal lamina stretches
45. Examination of the joint
detailed history & a thorough examination is needed
46. History
• Difficulty / pain when opening mouth,
chewing, talking
• Does your jaw get “stuck” or “locked” or “ go out”or feel stiff, tight
or tired
• Noises in the joint
• Pain in the ear, temple or cheek
• Frequent headaches, neckaches / toothaches
• Recent injury to your head, neck / jaw
47. examination
• Inspection – Facial appearance
Range of mandibular movement
Deviation
Deflection
• Palpation
• Load testing of the joint
• Auscultation : Joint sounds
• Intraoral examination
52. PALPATION
• Bimanually with index finger
• Lateral pole/head of the condyle
– preauricular region
• Posterior capsule – finger move towards ear
intra auricular method
53. LOAD TESTING OF THE JOINT
Load testing is mainly a means to palpate the head of the
condyle, the surface of the glenoid fossa and the tissue interposed
between them, except in case of a bone–bone contact.
54. • Bimanual mandibular manipulation
• Slight force applied by the fingers
• Increasing force to load – test the joints
• Discomfort – muscle incoordination
anteriorly displaced disc
58. Popping :
• Loud sound on opening, without stethoscope
Crepitus :
• Multiple gravel like sound – grating, complicated
• Fine crepitus: weak grating sound
mild bone – bone contact
• Coarse crepitus: strong grating sound
gross bone – bone contact
• Suggests degenerative joint disease
59. Intraoral examination
Signs of parafunction – Cheek biting
Linea alba
Occlusal wear
Tooth mobility
Gen. sensitivity to percussion
60. Imaging of the TMJ
• Is necessary to supplement information from examination
• Purpose –
• evaluate the integrity and relationships of the hard and soft tissues
• confirm the extent or stage of progression of the disease
• evaluate the effects of treatment
63. Transcranial Projection
• Gross osseous changes on the lateral aspects of the condyle
and temporal component
• Displaced condylar fractures
• Range of motion
CLOSED POSITION OPEN POSITION
64. Transpharyngeal Projection (maximal opening)
• Sagittal view of the medial pole of the condyle
• Erosive changes of the condyle
Transpharyngeal projection
showing the condyle (C) at
the articular eminence (E).
The zygomatic arch (Z) is
superimposed over the
glenoid fossa.
(C)
(Z)
(E)
65. Transorbital Projection
• Anterior view of the TMJ
• Mediolateral dimension of the
articular eminence, condylar
neck and head
• Condylar neck fractures
• Adjunct to transcranial and
transpharyngeal projections
Transorbital view showing the condyle
(arrows) below the articular eminence. The
mastoid process partly obscures the articulating
surface on the mediosuperior aspect.
66. Computed Tomography
• Information regarding 3D shape and internal structure of the
osseous component or surrounding soft tissues
Normal TMJ CT showing normal disk
posterior and superior to condyle (C).
Displaced meniscus (arrow) anterior to the
condyle.
67. MRI
• Imaging of articular disc
• Medial disc displacements are best detected using MRI
Normal
joint
Anterior disc
displacement
69. Classification
I. Developmental disturbances of the TMJ
• Aplasia of the mandibular condyle
• Hypoplasia
• Hyperplasia
II. Traumatic disturbances of the TMJ
• Luxation & subluxation
• Ankylosis
• Injuries of the Articular disc
• Fractures of the condyle
70. III. Inflammatory disturbances of the TMJ
• Arthritis due to specific infection
• Rheumatoid arthritis
• Osteoarthritis
IV. Neoplastic disturbances of the TMJ
V. Extra – articular disturbances of the TMJ
• TMJ syndrome
• Langerhans cell histiocytosis
• Hand – schuller christian disease
• Eosinophilic granuloma
71. Myofascial pain dysfunction syndrome
• It is a chronic disorder characterized by pain, clicking, trismus
& absence of radiological abnormalities.
• Myofascial pain may occur in any skeletal muscle of the body
including the muscle of mastication.
• Also known as Costen’s syndrome
72. Etiology
• Skeletal muscle spasm
• Psychological cause
• Irregularities in occlusion
• Decreased/increased vertical dimension
• Parafunctional habits
• Trauma to joint
• Sleep disturbances
• Hyper mobility of joint
73. Clinical features
• Age: commonly 20-40 years
• Females > males
• Laskin’s 4 cardinal signs:
1. Unilateral dull pain
2. Muscle tenderness
3. Clicking/ popping joint
4. Limitation of jaw function, deviation of the mandible on
opening
75. Disc Dislocation With Reduction
• Common disorder
• Disc displaced anteriorly
• On opening, a "pop" or
"click" heard and usually
felt – "Reducing the joint”
• Upon closing, the condyle
will slide off the back of the disc, hence another "click"
or "pop" heard
76. • Management:
1. No pain – no therapy
2. Flat–plane stabilization splint
3. Anterior repositioning splints
77. Disc Dislocation Without Reduction
• Closed lock
• Mouth opening is limited
• Disc dislocated anteromedially
from condyle does not return
to normal position with
condylar movement
• No "pop" or "click" sound
on opening
• Sometimes there is a tear or perforation of the disc.
78. • Management :
1. Manual manipulation
2. Exercises to increase range of motion
79. Subluxation
• Hypermobility
• condyle moves anterior to crest of articular eminence.
Cause: result of anatomic form of fossa,
steep short posterior slope of eminence,
longer flat anterior slope
• Results when disc is maximally rotated on condyle before full
translation.
80. • History- Patient reports a locking sensation when ever mouth is
opened too widely.
• Clinical features - Sudden jump of condyle forward with a ‘thud’
sensation.
• Treatment – Eminectomy- reducing steepness of eminence.
81.
82. Ankylosis
• Abnormal immobility of the joint.
• Two types- fibrous and bony
• Fibrous - occurs between
condyle and disc /
disc and fossa
• Bony - condyle and fossa.
83. Aplasia of condyle
• Condylar aplasia or failure of development of the mandibular condyle
may occur unilaterally or bilaterally.
• Frequently associated with other anatomically related defects such as
defective or absent external ear, an underdeveloped mandibular ramus
or macrostomia.
• If the condylar aplasia is unilateral , there is obvious facial asymmetry,
and both occlusion and mastication may be altered.
TREATMENT - osteoplasty in severe cases.
84. • Cause: most commonly- hemarthrosis secondary to trauma.
• History – report limited mouth opening without any pain.
• Clinical features
• Facial asymmetry
• Deviation to affected side
• Hypoplasia
• Limited mouth opening
• Treatment: Arthroscopic surgery
85. Ankylosis
• Causes-traumatic injuries and infections in and about the
joint,abnormal intrauterine development birth injury, congenital
syphilis, primary inflammation of joint (rheumatoid arthritis,
infectious arthritis) etc.
• Clinical features-The patient may or may not be able to open his
mouth to any appreciable extent depending on the type of
ankylosis.
• In complete ankylosis there is a bony fusion with absolute limitation
of motion. In unilateral ankyloses occuring at an early age, the chin
is displaced laterally and backward on the affected side because of
failure of development of mandible.
Treatment-Gap Arthroplasty,Osteotomy.
86. Hypoplasia of condyle
• Underdevelopment or defective formation of mandibular
condyle may be congenital or acquired.
• Congenital hypoplasia is of idiopathic origin.
• Acquired hypoplasia may be due to forceps deliveries,
external trauma to condylar area in infants and children,
infection spreading locally from the dental area
• Unilateral involvement is most common type
87. Hyperplasia of condyle
• Unilateral enlargement of the condyle.
• The cause of this condition is unknown. The patients usually
exhibit unilateral, slowly progressive elongation of the face with
deviation of the chin away from the affected side.
• Treatment - resection of the condyle
88. Luxation& Subluxation
• Dislocation of the condyle occurs when the head of
the condyle moves anteriorly over the articular
eminence into such a position that it cannot be
returned voluntarily to its normal position.
• Luxation may be acute owing to a sudden traumatic
injury resulting in the fracture of the condyle or more
frequently only in a stretching of capsule, usually at
the point of attachment for the external pterygoid
muscle into the capsule.
89. AGE CHANGES OF TMJ
• Flattened condyle
• Thinning of the disc
• Fibrotic synovial folds
• Thickening of the blood vessel walls
90. • Decrease the number of nerves
• Osteoporosis of the condyle bone
• Thickening of the fibrous covering of the condyle
• Thinning of the cartilaginous zone of condyle
92. References
P. Okeson. 5th Edition. Management of temporomandibular disorders and occlusion. Mosby Year Book.
Greenberg MS, Glick M. 10th Edition. Burket’s Oral Medicine – Diagnosis and Treatment. Elsevier.
Gray’s anatomy. 39th edition. Anatomical basis of clinical practice.
Sarnat BG, Laskin DM. 4th Edition. The Temporomandibular Joint: A Biological Basis for Clinical Practice.
Saunders.
Balaji SM, Text book of Oral & Maxillofacial Surgery. Elsevier.
White SC, Pharoah MJ. 4th Edition. Oral Radiology, Principles and Interpretation.
Shafers .5th edition. Text book of oral pathology. Elsevier .
B.D Chaurasia Text Book Of anatomy.
TORA TORA Text Book OF Anatomy.
Orbans Oral histiology and embryology.
Significance- without asso tenderness of masticatory muscles, tenderness in d joint identifies inflammation,
(pg 488 carranza)
(pg 488 carranza)
Lippincott
Pic from carranza
Lippincott
Pic from carranza
Lippincott
Images r obtained in both clos n open…
TMD as a collective term embracing a number of clinical problems that involve the masticatory musculature, the temporpmandibular joint and associated structures or both
Based on etiology
Upon clenching, the condyle compresses the bilaminar area, and the nerves, arteries and veins against the temporal fossa, causing pain and inflammation.