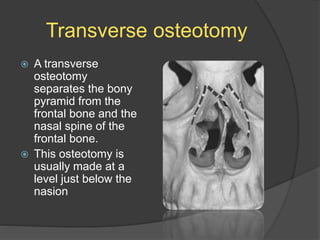
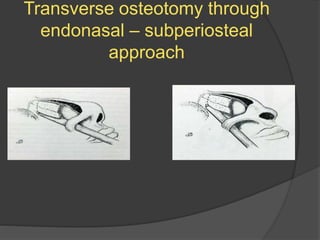
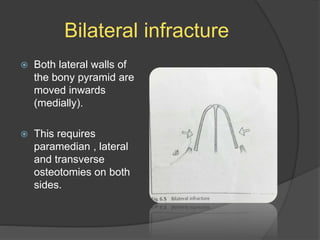
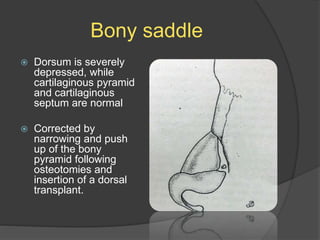
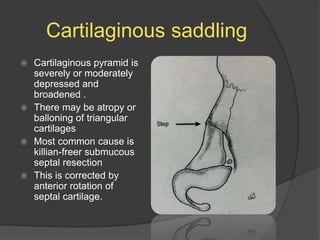
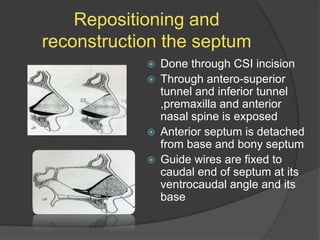
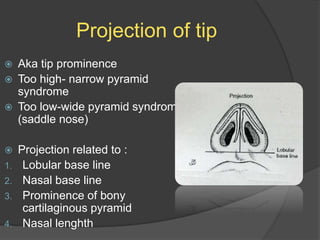
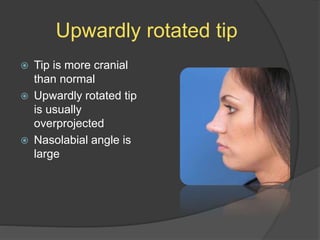
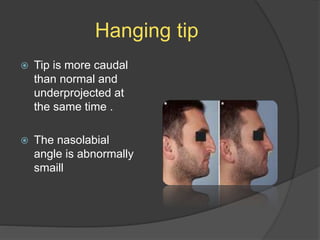
Downloaded 1,033 times
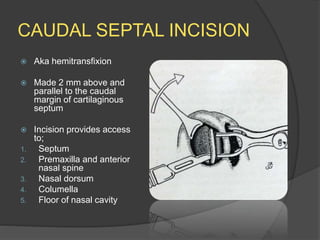
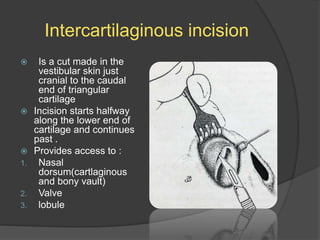
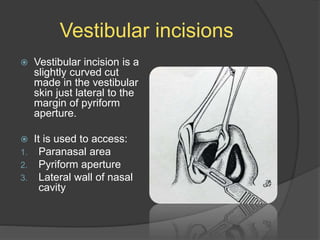
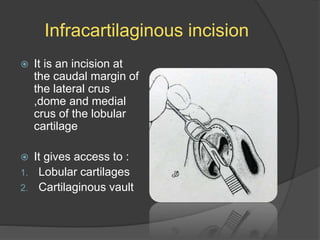
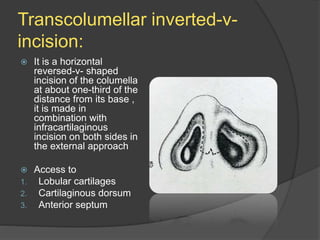
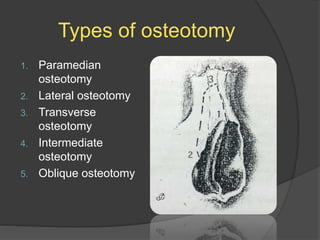
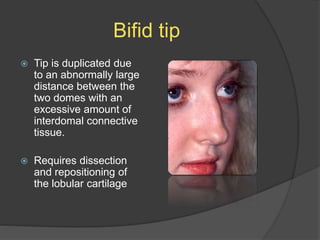
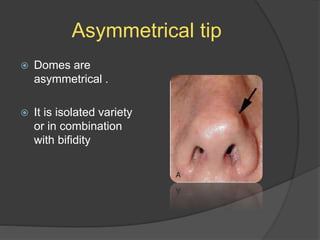
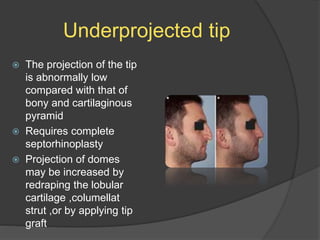
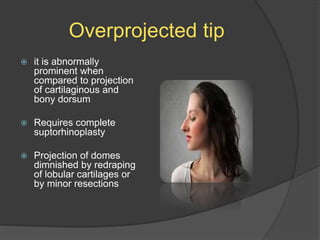
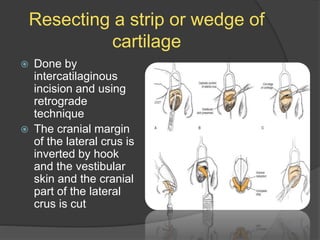
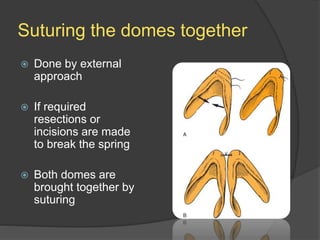
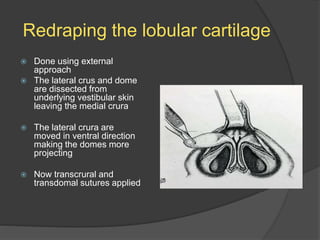
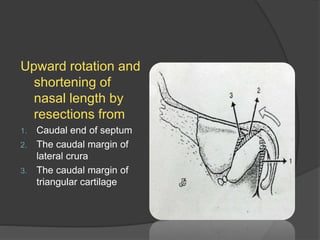
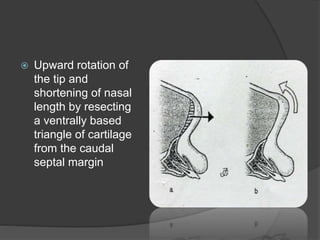
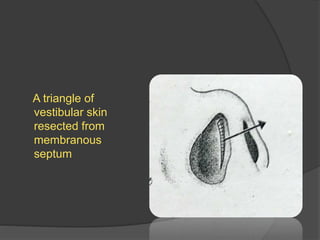
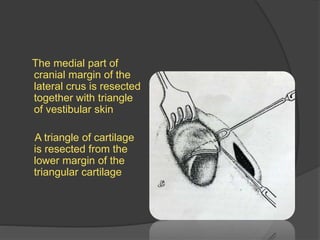

This document discusses various incisions and techniques used in rhinoplasty surgery. It describes the main incisions used including caudal septal, intercartilaginous, vestibular, infracartilaginous, and transcolumellar incisions. It then discusses techniques for accessing and mobilizing the bony nasal pyramid including different types of osteotomies. Other topics covered include hump removal, saddle nose correction, tip surgery, and correcting various tip abnormalities.












































































