Downloaded 61 times
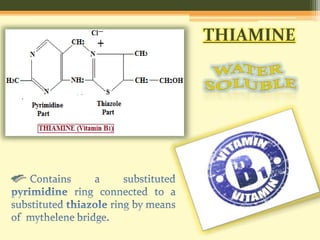

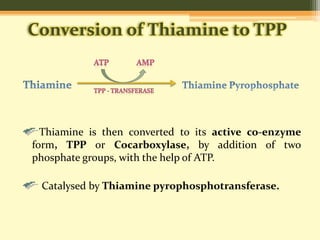







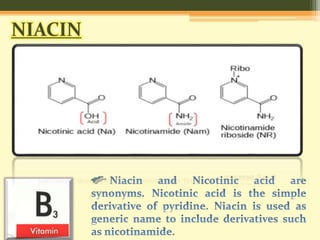

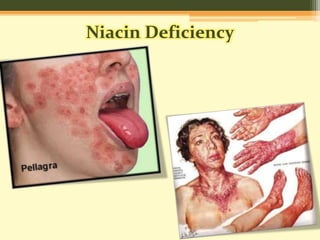



The document discusses thiamine and niacin, their sources, absorption, metabolism, and biochemical roles in the body. Thiamine occurs in plant seeds and is crucial for converting pyruvate to acetyl CoA, while niacin is important for metabolic coenzymes NAD and NADP, involved in various enzymatic reactions. Both vitamins are vital for proper bodily functions, and deficiencies can lead to significant health issues, including symptoms like dermatitis and neurological effects.