
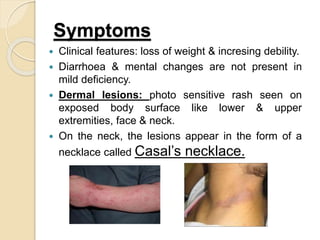


Vitamin B3, also known as niacin, is an essential vitamin that plays a key role in many metabolic processes in the body. It is found in a variety of foods like meat, fish, eggs, nuts, and whole grains. A deficiency in niacin can cause pellagra, with symptoms of dermatitis, diarrhea, dementia, and even death. Treatment involves increasing dietary intake of niacin through foods or supplements. Maintaining a balanced diet with adequate protein and B vitamins can help prevent niacin deficiency diseases.















































