Downloaded 65 times




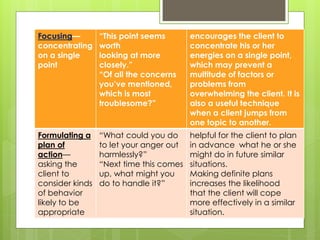
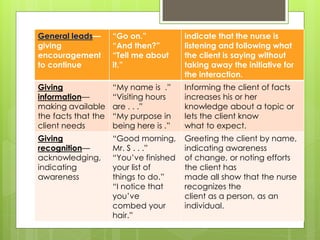
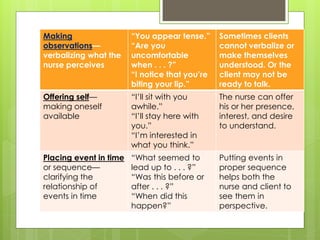
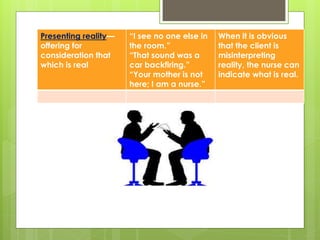

Therapeutic communication is an interpersonal interaction between a nurse and client where the nurse focuses on the client's needs to effectively exchange information. The goals of therapeutic communication are to establish a relationship with the client, identify their main concerns, and assess their perceptions in order to facilitate expression of emotions, teach self-care skills, recognize needs, and guide the client towards an action plan. Therapeutic communication techniques used by nurses include active listening, making observations, asking open-ended questions, and providing feedback to understand the client's perspective and address their needs.



















































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)









