Download as PDF, PPTX



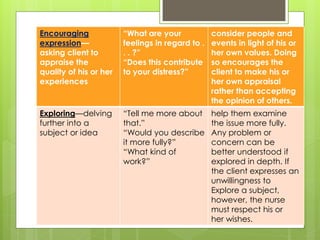
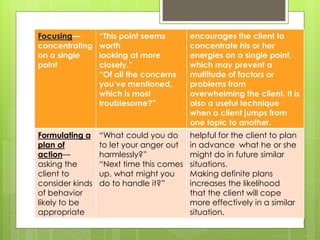
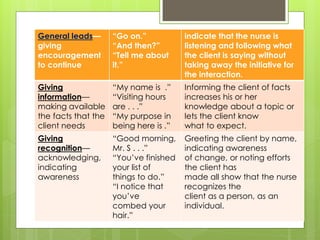
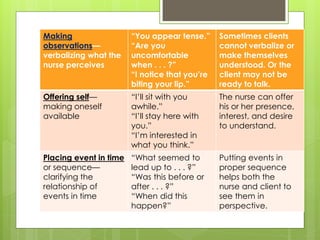

Therapeutic communication is an interpersonal interaction between a nurse and client that focuses on understanding and addressing the client's needs. The goals are to establish a relationship, identify concerns, assess perceptions, facilitate expression of emotions, teach self-care skills, recognize needs, and guide the client towards a plan of action. Therapeutic communication uses both verbal and nonverbal elements, and techniques include active listening, making observations, exploring topics in depth, focusing on key points, and formulating plans with the client. Conditions like values, culture, age, and environment can all affect communication between individuals.











































































































