NURSE – CLIENTINTERACTION
(COMMUNICATION)
COMMUNICATION : is the process that people use to
exchange information.
Messages are simultaneously sent and received on two
levels:
Verbally through the use of words
Non- verbally by behaviors that accompany the words.
3.
THERAPEUTIC COMMUNICATION
Isan interpersonal interaction between the nurse and
client during which the nurse focuses on the client’s
specific needs to promote an effective exchange of
information.
4.
THERAPEUTIC COMMUNICATION CAN
HELPNURSES TO ACCOMPLISH GOALS:
1. Establish a therapeutic nurse- client
relationship
2. Identify needs
3. Assess the client’s perception of the proble
4. CATHARSIS
5. Implement intervention
5.
TO HAVE EFFECTIVETHERAPEUTIC
COMMUNICATION THE NURSE MUST
CONSIDER:
Privacy and Respect of Boundaries
Use of Touch
Active listening and observation
6.
1. PRIVACY ANDRESPECT
BOUNDARIES
Privacy is desirable but not always possible in
Therapeutic Communication.
An interview or conference room is optimal
7.
BOUNDARIES
PROXEMICS: is thestudy of distance
zones between people during communication.
People feel more comfortable with smaller distance
when communicating with someone they know rather
than strangers.
4 Distance Zones:
1. Intimate
2. Personal
3. Social
4. Intimate
8.
4 Distance Zones:
1.Intimate zone ( 0 – ½ feet) : this amount of space is
comfortable for parents with young children,
people who mutually desire personal contact,
or people whispering.
2. Personal zone (1/2 – 4 feet) : this distance is
comfortable between family and friends who are talking.
9.
3. Socialzone (4 to 12 feet): this distance is
acceptable for communication in social, work, and
business settings.
4. Public zone (12 to 25 feet): this is acceptable
distance between a speaker and an audience, small
groups, and other informal functions.
10.
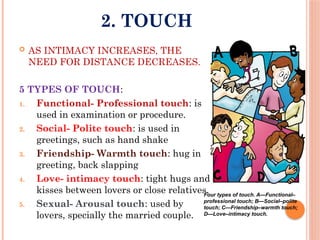
2. TOUCH
ASINTIMACY INCREASES, THE
NEED FOR DISTANCE DECREASES.
5 TYPES OF TOUCH:
1. Functional- Professional touch: is
used in examination or procedure.
2. Social- Polite touch: is used in
greetings, such as hand shake
3. Friendship- Warmth touch: hug in
greeting, back slapping
4. Love- intimacy touch: tight hugs and
kisses between lovers or close relatives.
5. Sexual- Arousal touch: used by
lovers, specially the married couple.
Four types of touch. A—Functional–
professional touch; B—Social–polite
touch; C—Friendship–warmth touch;
D—Love–intimacy touch.
11.
3. ACTIVE LISTENINGAND
OBSERVATION
To receive the sender’s simultaneous messages, the
nurse must use active listening and active
observation.
Active listening
Active observation
13.
COMMON MISCONCEPTIONOF STUDENTS
learning the art of THERAPEUTIC
COMMUNICATION = is that they always must be
ready with questions the instant the client has
finished speaking.
They are constantly thinking ahead regarding the
next question rather than actively listening to
what the client is saying.
USING THERAPEUTIC COMMUNICATION
TECHNIQUES:
The choice of technique depends on the intent of
the interaction and the client’s ability to
communicate verbally.
Techniques such as exploring, focusing,
restating, and reflecting encourage the client
to discuss his/her feelings or concerns in more
depth.
16.
THERAPEUTIC
COMMUNICATION TECHNIQUES:
1. Accepting: indicating reception
Ex. “yes” “I follow what you said.” Nodding
2. Broad opening: allowing the client to take the
initiative in introducing the topic.
Ex. “Is there something you’d like to talk about?”
“Where would you like to begin?”
3. Consensual validation: searching to
mutual understanding, for accord in the meaning of the
words.
Ex. “ Tell me whether my understanding of it agrees
with yours.”
17.
4. Exploring: delvingfurther into a subject or
idea.
Ex. “ Tell me more about that.” “Would you describe it
more fully?”
5. Focusing: concentrating on a single point.
Ex. “This point seems worth looking at more closely.”
18.
A FEMALE VICTIMOF A SEXUAL ASSAULT IS BEING SEEN IN
THE CRISIS CENTER FOR A THIRD VISIT. SHE STATES THAT
ALTHOUGH THE RAPE OCCURRED NEARLY 2 MONTHS AGO,
SHE STILL FEELS “AS THOUGH THE RAPE JUST HAPPENED
YESTERDAY.” THE NURSE WOULD RESPOND BY STATING:
A. “What can you do to alleviate some of your
fears about being assaulted again?”
B. “Tell me more about those aspects of the rape
that cause you to feel like the rape just
occurred.”
C. “In time, our goal will be to help you move on
from these strong feelings about your rape.”
D. “In reality, the rape did not just occur. It has
been over two months now.”
19.
6. General leads:giving encouragement to
continue.
Ex. “Go on” “and then?” “Tell me about it.”
7. Giving information: making available the
facts that the client needs.
Ex. “My name is....” “Visiting hours are...” “My purpose
in being here is.....”
20.
A 4-YEAR-OLD CHILDWHO WAS RECENTLY
HOSPITALIZED IS BROUGHT TO THE CLINIC BY HIS
MOTHER FOR A FOLLOW-UP VISIT. THE MOTHER
TELLS THE NURSE THAT THE CHILD HAS BEGUN TO
WET THE BED EVER SINCE THE CHILD WAS BROUGHT
HOME FROM THE HOSPITAL. THE MOTHER IS
CONCERNED AND ASKS THE NURSE WHAT TO DO. THE
APPROPRIATE NURSING RESPONSE WOULD BE:
A. “You need to discipline the child.”
B. “This is a normal occurrence following
hospitalization.”
C. “We need to discuss this behavior with
the physician.”
D. “The child probably has developed a
urinary tract infection.”
21.
8. Giving recognition:acknowledging,
indicating awareness: “Good morning, Mr. S.......” “ I
notice that you’ve combed your hair.”
9. Making observations: verbalizing what
the nurse perceives.
Ex. “You appear tense.” “ I notice you’re biting your
lip.”
10. Offering self: making oneself available.
Ex. “ I’ll sit with you awhile.”
22.
A NURSE OBSERVESAN ANXIOUS CLIENT
BLOCKING THE HALLWAY, WALKING THREE
STEPS FORWARD AND THEN TWO STEPS
BACKWARD.OTHER CLIENTS ARE AGITATED
TRYING TO GET PAST. THE NURSE
INTERVENES BY:
A. Standing alongside the client and saying,
“You’re very anxious today.”
B. Stopping the behavior and saying: “You’re
going to get exhausted.”
C. Taking the client to the TV lounge and saying,
“Relax and watch television now.”
D. Walking alongside the client and saying, “
You’re not going to get anywhere very fast
doing this.”
23.
A MALE CLIENTDIAGNOSED WITH CATATONIC
STUPOR DEMONSTRATES SEVERE WITHDRAWAL
BY LYING ON THE BED WITH THE BODY PULLED
INTO A FETAL POSITION. THE NURSE PLANS TO:
A. Leave the client alone and intermittently check on
him.
B. Take the client into the day room with other
clients so they can help watch him.
C. Sit beside the client in silence and occasionally ask
open-ended questions.
D. Ask direct questions to encourage talking.
24.
11. Presenting reality:offering for
consideration that which is real.
Ex. “ I’ll see no one else in the room.”
16. Reflecting: directing client actions. Thoughts,
and feelings back to client.
Ex. Client: “do you think I should tell the doctor....?
Nurse: “do you think you should?”
25.
COMMUNICATION TECHNIQUE
SHOULD THENURSE USE WHEN
COMMUNICATING WITH A CLIENT
WHO IS EXPERIENCING AUDITORY
HALLUCINATIONS?
A "My sister has the same diagnosis as you and
she also hears voices."
B "I understand that the voices seem real to you,
but I do not hear any voices."
C "Why not turn up the radio so that the voices
are muted.”
D "I wouldn't worry about these voices. The
medication will make them disappear.
26.
Auditory hallucinations,the most common type,
involve hearing sounds, most often voices, talking
to or about the client.
Command hallucinations are voices demanding
that the client take action, often to harm self or
others, and are considered dangerous.
The nurse reorients the patient to reality and
assesses for the presence of such hallucinations to
ensure safety.
Address him by name to ask him if he is hearing
voices again
“I do not hear the voice you say you hear.”
27.
12. Restating: repeatingthe main idea expressed.
Ex. Client: “ I can’t sleep. I stay awake all the night.”
Nurse: “you have difficulty sleeping.”
13. Reflecting—directing client actions, thoughts, and
feelings back to client
Client: “Do you think I should tell the doctor . . . ?”
Nurse: “Do you think you should?”
Client: “My brother spends all my money and then has nerve to ask for
more.”
Nurse: “This causes you to feel angry?”
28.
A CLIENT SAYSTO THE NURSE, “I’M GOING
TO DIE AND I WISH MY FAMILY WOULD
STOP HOPING FOR A CURE! I GET SO
ANGRY WHEN THEY CARRY ON LIKE THIS!
AFTER ALL, I’M THE ONE WHO’S DYING.”
THE NURSE MAKES WHICH THERAPEUTIC
RESPONSE TO THE CLIENT?
A. You’re feeling angry that your family continues
to hope for you to be cured?”
B. “I think we should talk more about your anger
at your family.”
C. “Well, it sounds like you’re being pretty
pessimistic. After all, years ago, people died of
pneumonia.”
D. “Have you shared your feelings with your
family?
30.
AVOIDING NONTHERAPEUTIC
COMMUNICATION
Incontrast, there are many therapeutic
techniques that nurses should avoid. These
responses cut off communication and make
it more difficult for the interaction to
continue.
Responses such as “Everything will work out”
or “May be tomorrow will be a better day”
may be intended to comfort the client, but
instead may impede the communication process.
31.
NONTHERAPEUTIC
COMMUNICATION TECHNIQUES:
1.Advising: telling the client what to do.
Ex. “ I think you should...”
2. Agreeing: indicating accord with the client.
Ex. “That’s right.”
3. Belittling feelings expressed: misjudging the
degree of the client’s discomfort.
Ex. Client: “ I have nothing to live for... I wish I
was dead.” Nurse: “ Everybody gets down in the
dumps.” or “I’ve felt that way myself.”
32.
4. Challenging:demanding proof from client.
Ex. “But how can you be president of the United
State?” “If you’re dead, why is you heart beating?”
5. Defending: attempting to protect someone or
something from verbal attack.
Ex. “This hospital has a fine reputation.” “ I’m sure
your doctor has your best interests in mind.’
33.
6. Disagreeing:opposing the client’s ideas.
Ex. “that’s wrong.”
7. Disapproving: denouncing the client’s behavior or
ideas.
Ex. “That’s bad” “I’d rather you wouldn’t
8. Giving approval: sanctioning the client’s behavior
or ideas.
Ex. “That’s good.” “I’m glad that...’
34.
9. Interpreting:asking to make conscious that which
is unconscious; telling the client the meaning of his or
her experience.
Ex. “What you really mean is....” “Unconsciously you’re
saying....”
10. Probing: persistent questioning of the client.
Ex. “Now tell me about this problem. You know I have
to find out.”
35.
INTERPRETING SIGNALS OR
CUES
To understand what the client means, the nurse
watches and listens carefully for cues.
CUES: are verbal or nonverbal messages that
signal key words or issues for the client.
36.
NONVERBAL COMMUNICATION
SKILLS
Isbehavior that a person exhibits while
delivering verbal content.
It includes:
facial expression,
eye contact,
space ,
time,
boundaries, and
body movements.
37.
1. FACIAL EXPRESSION
The human face produces the most visible, complex,
and sometimes confusing nonverbal messages.
Facial movements connect with words to illustrate
meaning; this connection demonstrates the speaker’s
internal dialogue.
Facial expression can be
categorized into:
Expressive
Impassive
Confusing
39.
FACIAL EXPRESSION
often affectthe listener’s
response. The nurse should
identify the facial expression and
ask the client to validate nurse’s
interpretation of it.
Ex. “ you’re smiling, but I
sense you are very angry.”
40.
2. BODY LANGUAGE
Gesture, postures, movements,
and body positions.
Is a nonverbal form of
communication.
Closed Body Position
Accepting Body Position
41.
VOCAL CUES
Arenonverbal sound signals transmitted
along with the content: voice volume, tone,
pitch, intensity, emphasis, speed, and
pauses augment the sender’s message.
42.
EYE CONTACT
Theeyes have been called the mirror of the soul
because they often reflect our emotions.
Although maintaining good eye contact is usually
desirable, it is important that the nurse doesn’t
“STARE” at the client.
43.
SILENCE
Or longpauses in communication may indicate many
different things.
The client may be depressed
Sometimes pauses indicate the client is thoughtfully
considering the question before responding.
It is important to allow the client sufficient time
to respond, even if it seems like a long time.
THERAPEUTIC RELATIONSHIP
The nurse’srelationship with the
patient consists of a series of goal-
directed interactions through which
the nurse assesses patients’
problems, elicits patient input,
selects interventions, and evaluates
the effectiveness of care.
THERAPEUTIC RELATIONSHIP
Thenurse uses communication skills,
personal strengths, and
understanding of human behavior to
interact with the client.
The nurse must constantly focus on
the client’s needs not his/her own.
49.
COMPONENTS OF A
THERAPEUTICRELATIONSHIP
Trust
Genuine interest
Empathy
Acceptance
Positive regard
Self-awareness
Therapeutic use of self
50.
TRUST
Trust develops whenthe
client believes that the
nurse will be consistent in
his/her words and actions
and can be relied on to do
what he or she says.
EMPATHY
Is the abilityof the nurse to
perceive the meaning and feelings of
the client and to communicate that
understanding to the client.
It is considered one of the essential skills a nurse
must develop.
Being able to put himself/herself in the client’s
shoes
Ex. Empathy : “I see you are sad.... How can I
help you?”
Ex. Sympathy : “ I feel so sorry for you.”
53.
ACCEPTANCE
The nurse whodoes not become
upset or respond negatively to a
client’s outbursts, anger, or acting
out conveys acceptance to the client.
54.
The nursemust set boundaries in the nurse-
client relationship.
Ex. A client puts his arm around the nurse’s
waist.
An appropriate response would be what?
55.
POSITIVE REGARD
The nursewho appreciates the
client as a simple worth while
human being can respect the client
regardless of his or her behavior,
background, or lifestyle.
56.
SELF- AWARENESS
Beforethe nurse can begin to understand
clients, the nurse must know himself /herself.
Self – awareness: is the process of developing an
understanding of one own’s values, beliefs, thoughts,
feelings, attitude, motivations, prejudices, strengths,
and limitations and how these qualities affect others.
57.
THERAPEUTIC USE OFSELF
By developing self- awareness and
beginning to understand his/ her
attitudes, the nurse can begin to use
aspects of his/her personality,
experiences, values, feelings, intelligence,
needs, coping skills, and perceptions to
establish relationships with client.
Nurses use themselves as therapeutic tool to
establish therapeutic relationships with clients
and help clients grow, change, and heal.
Editor's Notes
#3 therapeutic communication techniques helps the nurse understand and empathize with the client’s experience.
All nurses need skills in therapeutic communication to effectively apply the nursing process and to meet standards of care for their client.
#4 4. Facilitate the client’s expression of emotions.
5. Teach the client and family necessary self-care skills.
6. Recognize the client’s needs.
7. Implement intervention designed to address the client’s needs.
8. Guide the client toward identifying a plan of action to a satisfying and socially acceptable resolution.
#6 The nurse needs to evaluate whether interacting in the client’s room is therapeutic.
Ex. If the client has difficulty maintaining boundaries or has been making sexual comments, then the client’s room is not the best setting.
#8 Both the client and the nurse can feel threatened, if one invades the other’s personal or intimate zone, which can result tension, irritability, fidgeting (uneasy, nervous) , or even flight.
When the nurse must invade the intimate or personal zone, the nurse should ask the client’s permission.
invasion of this intimate zone by anyone else is threatening and produces anxiety.
Examples occur when nurses are sit-
ting with a client, giving medications, or establishing an intravenous
infusion. Communication at a close personal distance can convey
involvement by facilitating the sharing of thoughts and feelings. On
the other hand, it can also create tension if the distance encroaches
on the other individual’s personal space
#11 Active listening : means refraining from other internal mental activities and concentrating exclusively on what the client says.
Active observation : means watching the speaker’s nonverbal action as he/ she communicates.
#13 The result can be that the nurse does not understand the client’s concerns, and the conversation is vague, superficial, and frustrating to both participants.
Recognize the issue that is most important to the client at this time.
Know what further questions to ask the client.
Use additional therapeutic communication techniques to guide the client to describe his /her perceptions fully.
Understand the client’s perceptions of the issue instead of jumping to conclusions.
Interpret and respond to the message objectively.
#14 nurse should use words that are clear as possible when speaking to the client so that the client can understand the message.
In concrete message , the words are explicit and need no interpretation.
Concrete questions, are clear, direct, and easy to understand.
Ex. "what health symptoms caused you to come to the hospital today?” or “ when was the last time you took your antidepressant medications?”
#16 Accepting- indicating reception
“Yes.”
“I follow what you said.”
Nodding
An accepting response indicates the nurse has heard and followed the train of thought.
Not the same as agreeing!
It does not indicate agreement but is nonjudgmental.
Facial expression, tone of voice, and so forth also must convey acceptance or the words will lose their meaning.
Broad openings— allowing the client to take the initiative in introducing the topic
“Is there something you’d like to talk about?”
“Where would you like to begin?”
Broad openings make explicit that the client has the lead in the interaction. For the client who is hesitant about talking, broad openings may stimulate him or her to take the initiative.
Consensual validation—searching for mutual understanding, for accord in the meaning of the words
“Tell me whether my understanding of it agrees with yours.”
“Are you using this word to convey that . . . ?”
For verbal communication to be meaningful, it is essential that the words being used have the same meaning for both (all) participants. Sometimes words, phrases, or slang terms have different meanings and can be easily misunderstood.
#17 Exploring—delving further into a subject or idea
“Tell me more about that.”
“Would you describe it more fully?”
“What kind of work?”
When clients deal with topics superficially, exploring can help them examine the issue more fully.
Any problem or concern can be better understood if explored in depth.
If the client expresses an unwillingness to explore a subject, however, the nurse must respect his or her wishes.
Focusing— concentrating on a single point
“This point seems worth looking at more closely.”
“Of all the concerns you’ve mentioned, which is most troublesome?”
The nurse encourages the client to concentrate his or her energies on a single point, which may prevent a multitude of factors or problems from overwhelming the client.
a useful technique when a client jumps from one topic to another.
#19 General leads— giving encouragement to continue
“Go on.”
“And then?”
“Tell me about it.”
General leads indicate that the nurse is listening and following what the client is saying without taking away the initiative for the interaction.
They also encourage the client to continue if he or she is hesitant or uncomfortable about the topic.
Giving information— making available the facts that the client needs
“My name is . . .”
“Visiting hours are . . .”
“My purpose in being here is . . .”
Informing the client of facts increases his or her knowledge about a topic or lets the client know what to expect.
The nurse is functioning as a resource person
Giving information also builds trust with the client.
#21 Giving recognition— acknowledging, indicating awareness
“Good morning, Mr. S . . .”
“You’ve finished your list of things to do.”
“I notice that you’ve combed your hair.”
Greeting the client by name, indicating awareness of change, or noting efforts the client has made all show that the nurse recognizes the client as a person, as an individual.
Such recognition does not carry the notion of value, that is, of being “good” or “bad.”
Making observations—
verbalizing what the nurse perceives
“You appear tense.”
“Are you uncomfortable when . . . ?”
“I notice that you’re biting your lip.”
Sometimes clients cannot verbalize or make themselves understood. Or the client may not be ready to talk.
Offering self— making oneself available
“I’ll sit with you awhile.”
“I’ll stay here with you.”
“I’m interested in what you think.”
“You must have misplaced it in your room. Let’s go and look for it together.”
The nurse can offer his or her presence, interest, and desire to understand. It is important that this offer is unconditional, that is, the client does not have to respond verbally to get the nurse’s attention.
#24 Presenting reality— offering for consideration that which is real
“I see no one else in the room.”
“That sound was a car backfiring.”
“Your mother is not here; I am a nurse.”
When it is obvious that the client is misinterpreting reality, the nurse can indicate what is real.
The nurse does this by calmly and quietly expressing the nurse’s perceptions or the facts not by way of arguing with the client or belittling his or her experience.
The intent is to indicate an alternative line of thought for the client to consider, not to “convince” the client that he or she is wrong.
#27 Restating— repeating the main idea expressed
Client: “I can’t sleep. I stay awake all night.”
Nurse: “You have difficulty sleeping.”
The nurse repeats what the client has said in approximately or nearly the same words the client has used.
This restatement lets the client know that he or she communicated the idea effectively.
This encourages the client to continue. Or if the client has been misunderstood, he or she can clarify his or her thoughts.
Reflecting—directing client actions, thoughts, and feelings back to client
Client: “Do you think I should tell the doctor . . . ?”
Nurse: “Do you think you should?”
Client: “My brother spends all my money and then has nerve to ask for more.”
Nurse: “This causes you to feel angry?”
Reflection encourages the client to recognize and accept his or her own feelings.
The nurse indicates that the client’s point of view has value, and that the client has the right to have opinions, make decisions, and think independently.
#37 Nonverbal communication
involves the unconscious mind acting out emotions related to the verbal content, the situation, the environment, and the relationship between the speaker and the listener.
#46 The nurse indicates interest in and acceptance of the client by facing and slightly leaning toward him or her while maintaining nonthreatening eye contact
#57 A client with mental illness can detect when someone is exhibiting dishonest or artificial behavior such as asking a question and then not waiting for the answer, talking over him or her, or assuring him/her everything will be all right.
#59 Avoiding judgment s of the person, no matter what the behavior, is acceptance.
This does not mean acceptance of inappropriate behavior but acceptance of the person as worthy.
#60 An appropriate response would be for the nurse to remove his hand and say, “john, do not place your hand on me. We are working in your relation with your girlfriend and that does not require you to touch me. Now, let’s continue.”
#61 Calling the client by name, spending time with the client, and listening and responding openly are measures by which the nurse conveys respect and positive regard to the client.









































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)















