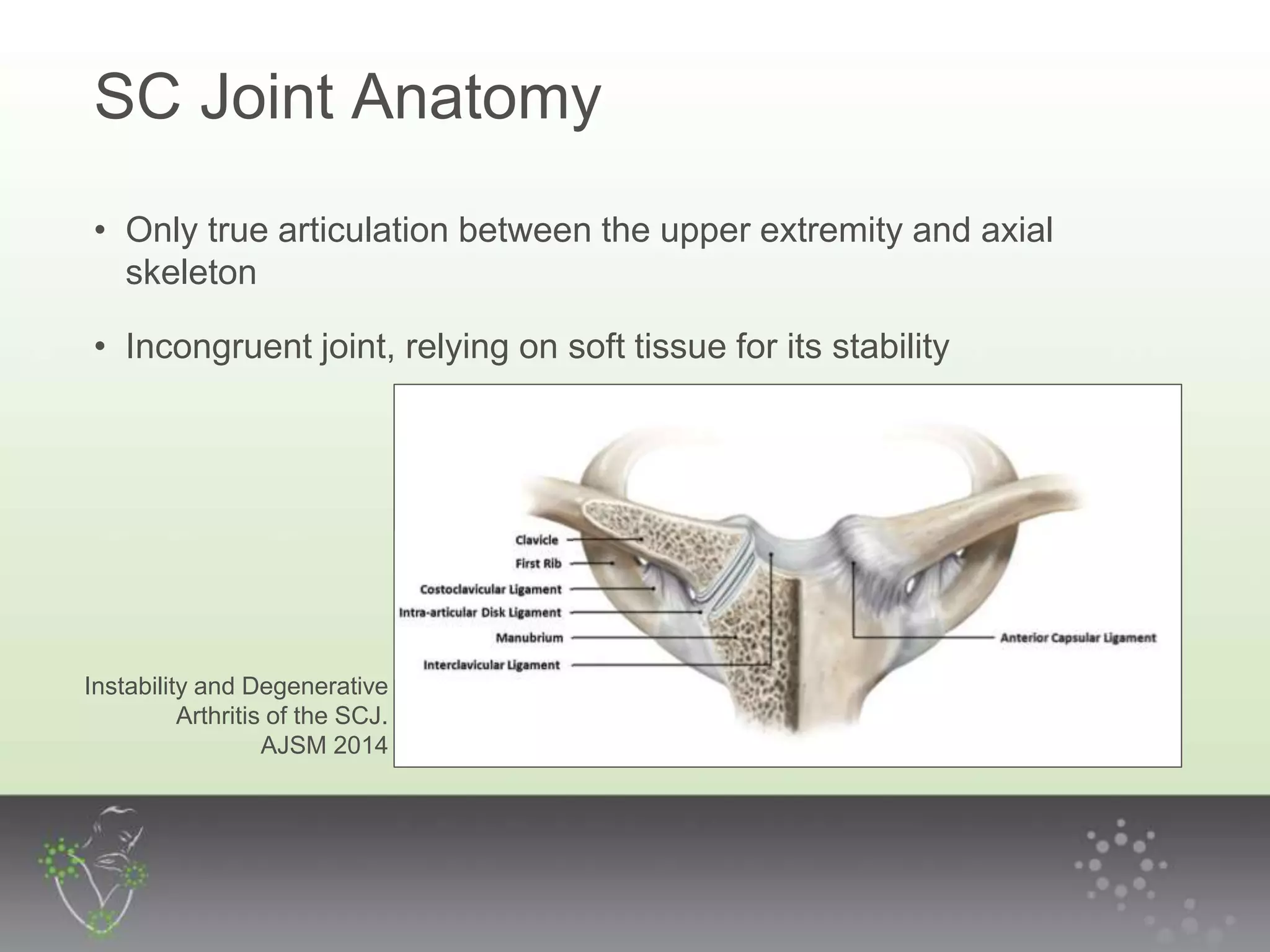
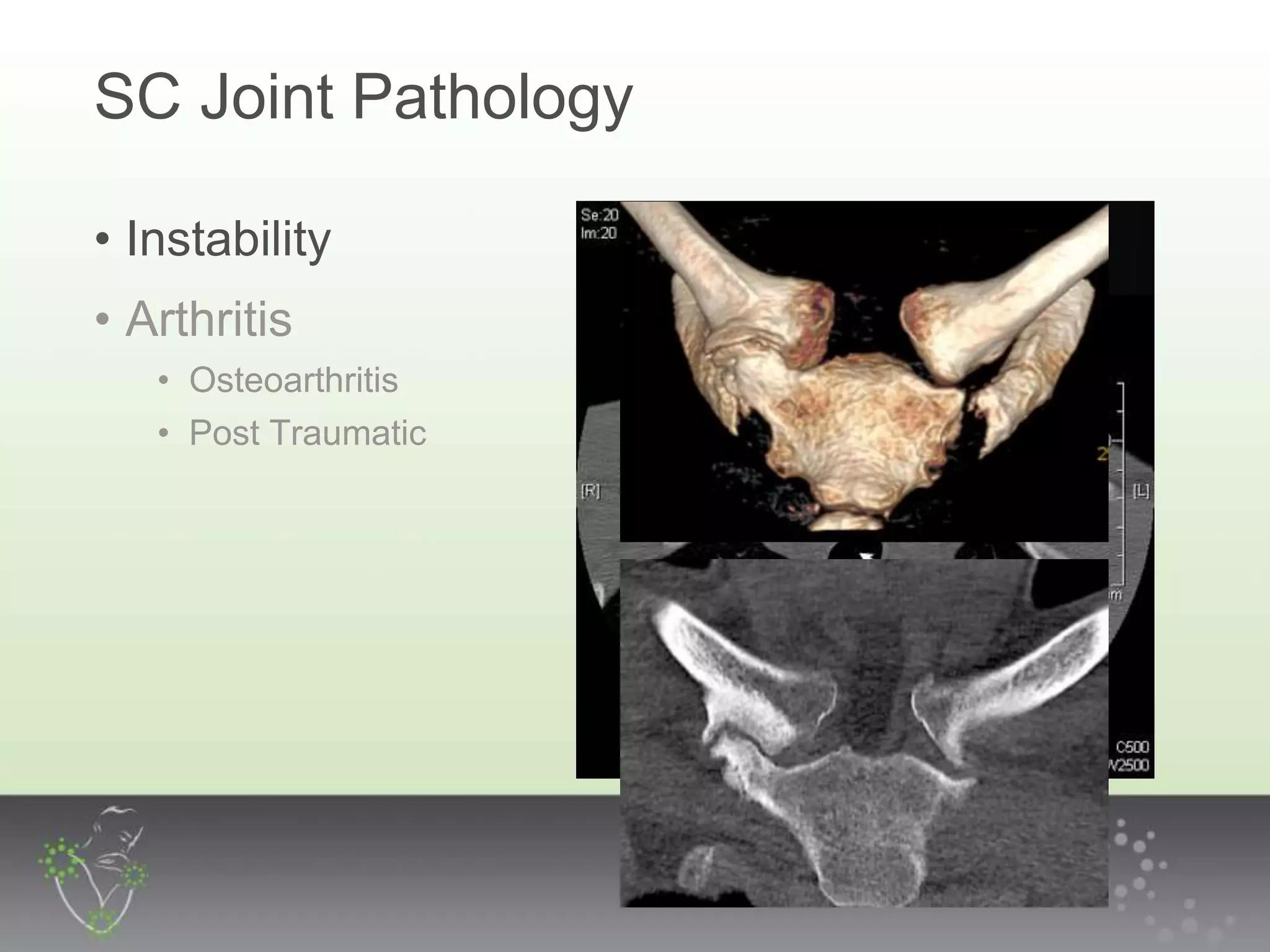
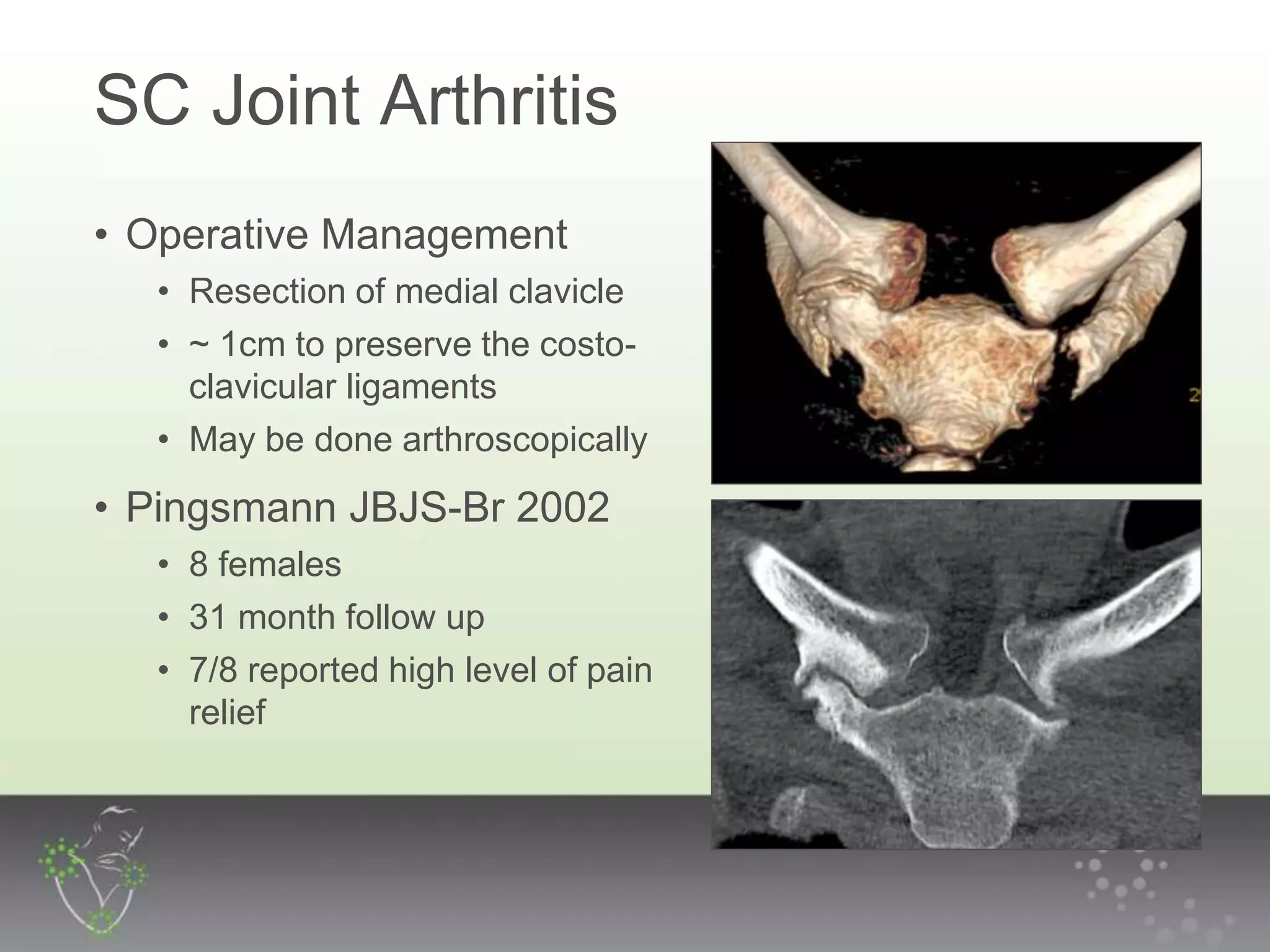
The document discusses the anatomy, pathology, and management of sternoclavicular joint (SCJ) injuries and arthritis, emphasizing the joint's reliance on soft tissue for stability. It outlines the classification and evaluation of SCJ instability along with treatment options, including non-operative and surgical methods, highlighting the need for careful management, especially in cases of acute dislocations. Overall, the majority of SCJ dislocations are anterior and may often be treated without surgery, although surgical intervention might be required for arthritis or severe cases.