The document provides an overview of forearm anatomy including bones (ulna, radius), joints (elbow, radioulnar), muscles, nerves, blood vessels, and approaches. Key points include:
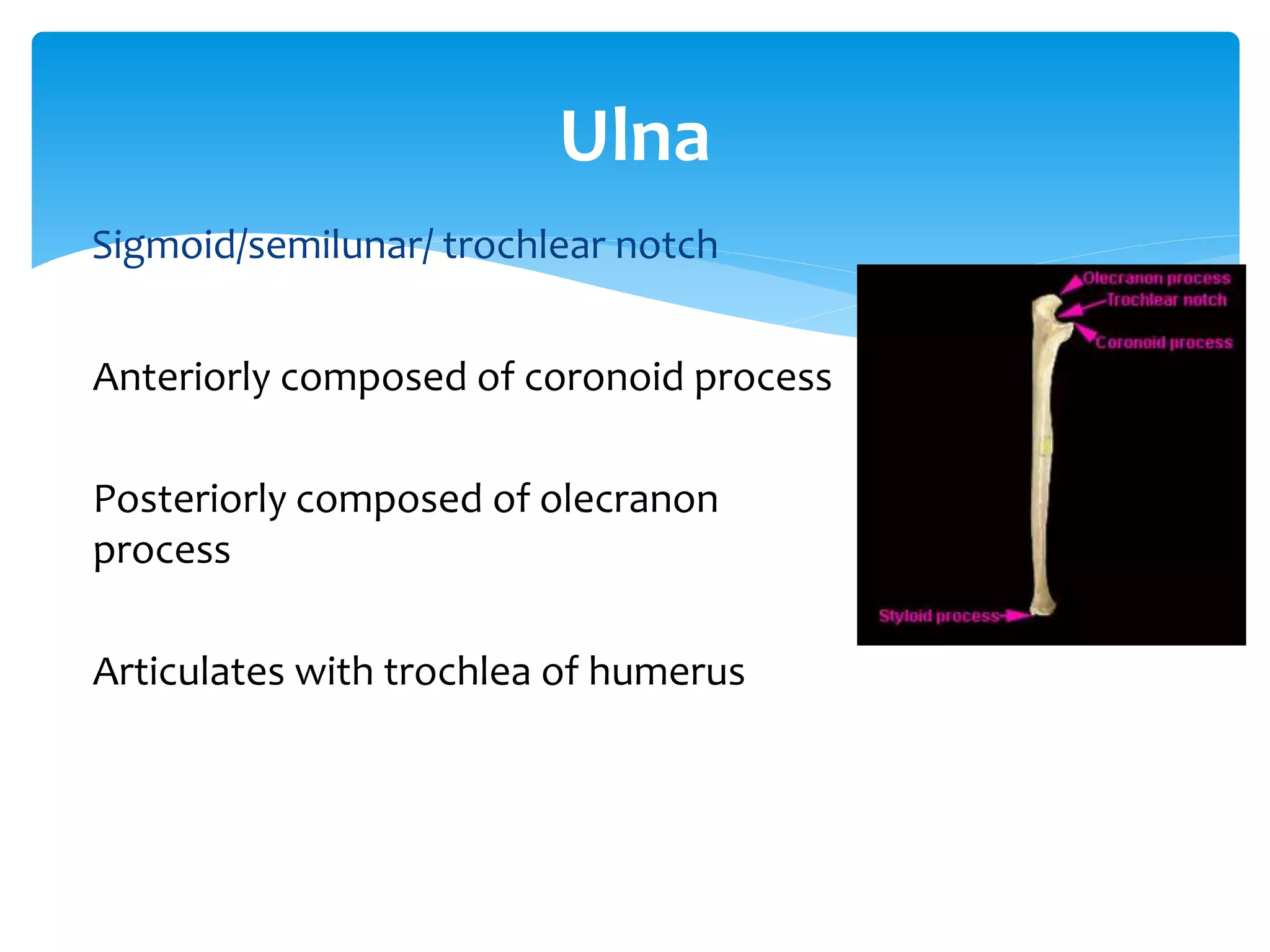
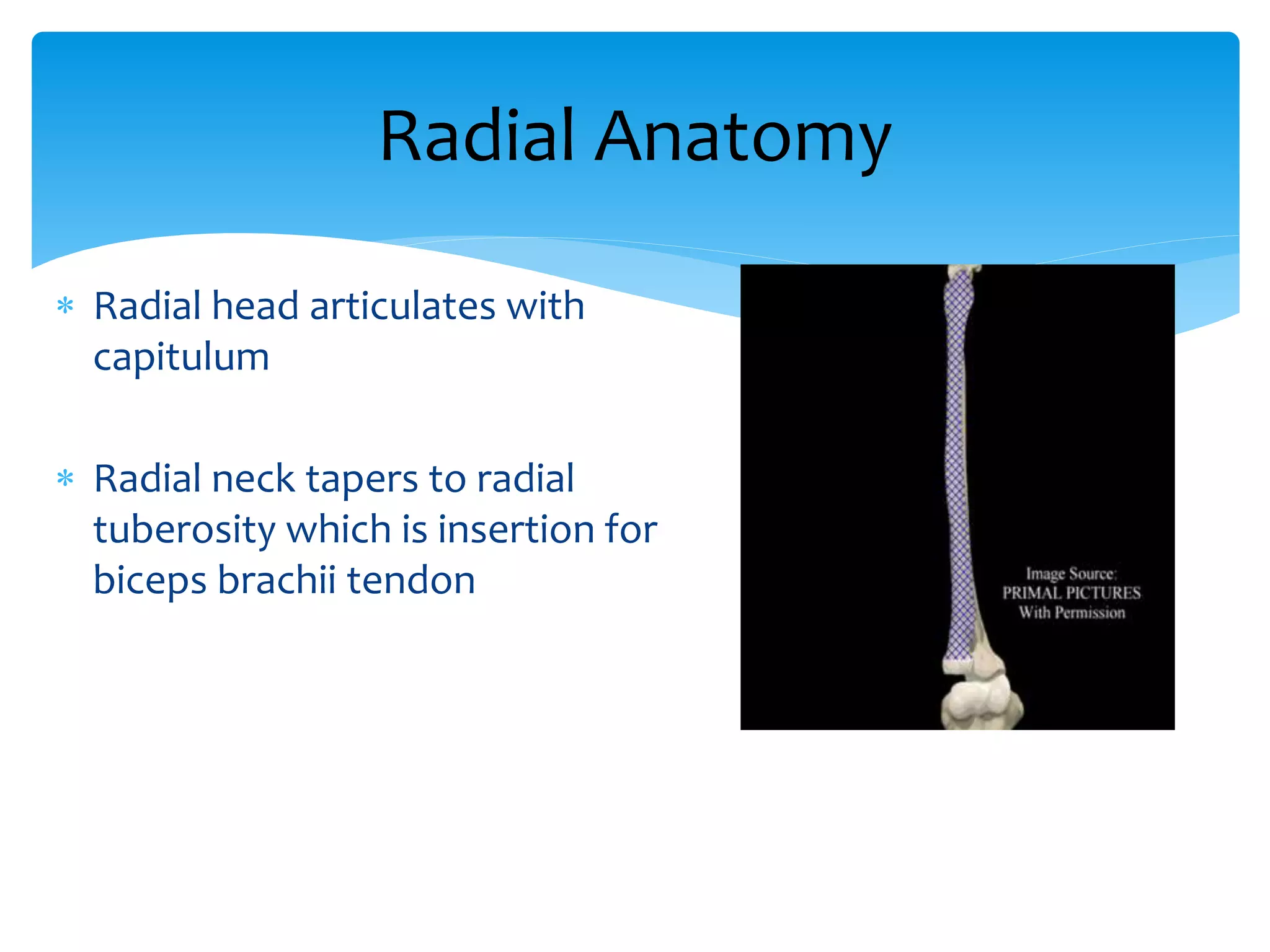
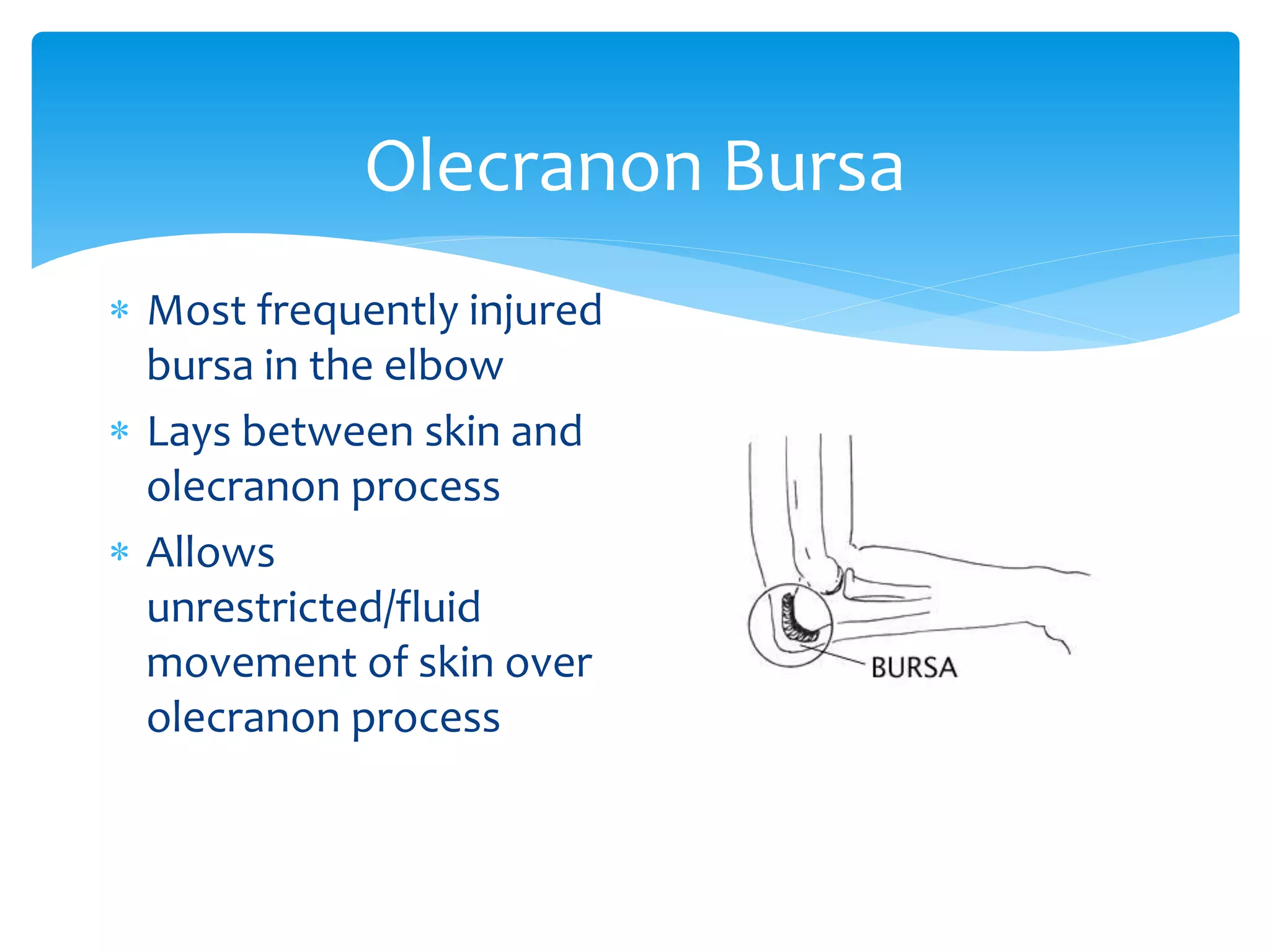
- The ulna articulates with the trochlea of the humerus at the elbow joint. The radial head articulates with the capitellum.
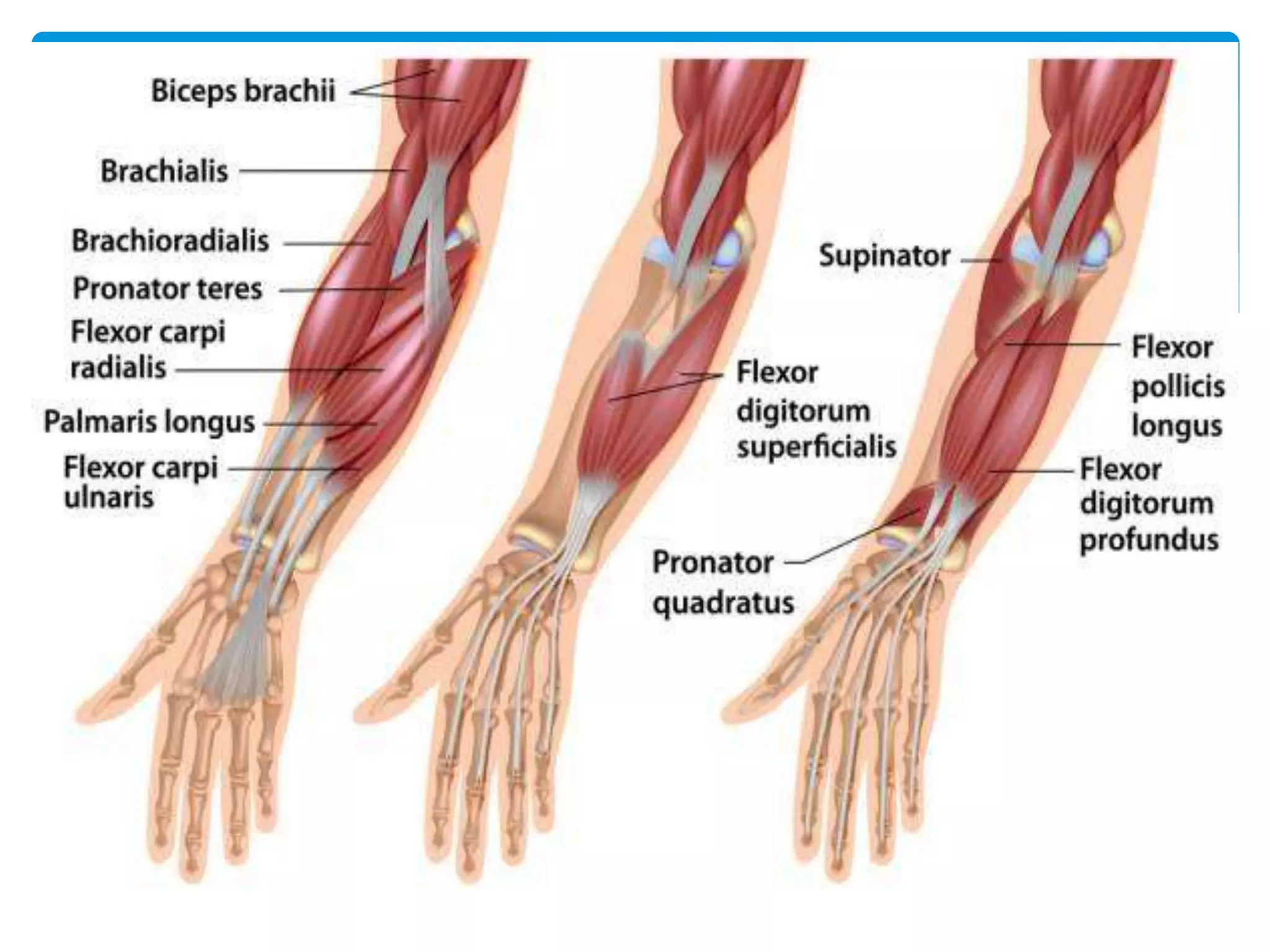
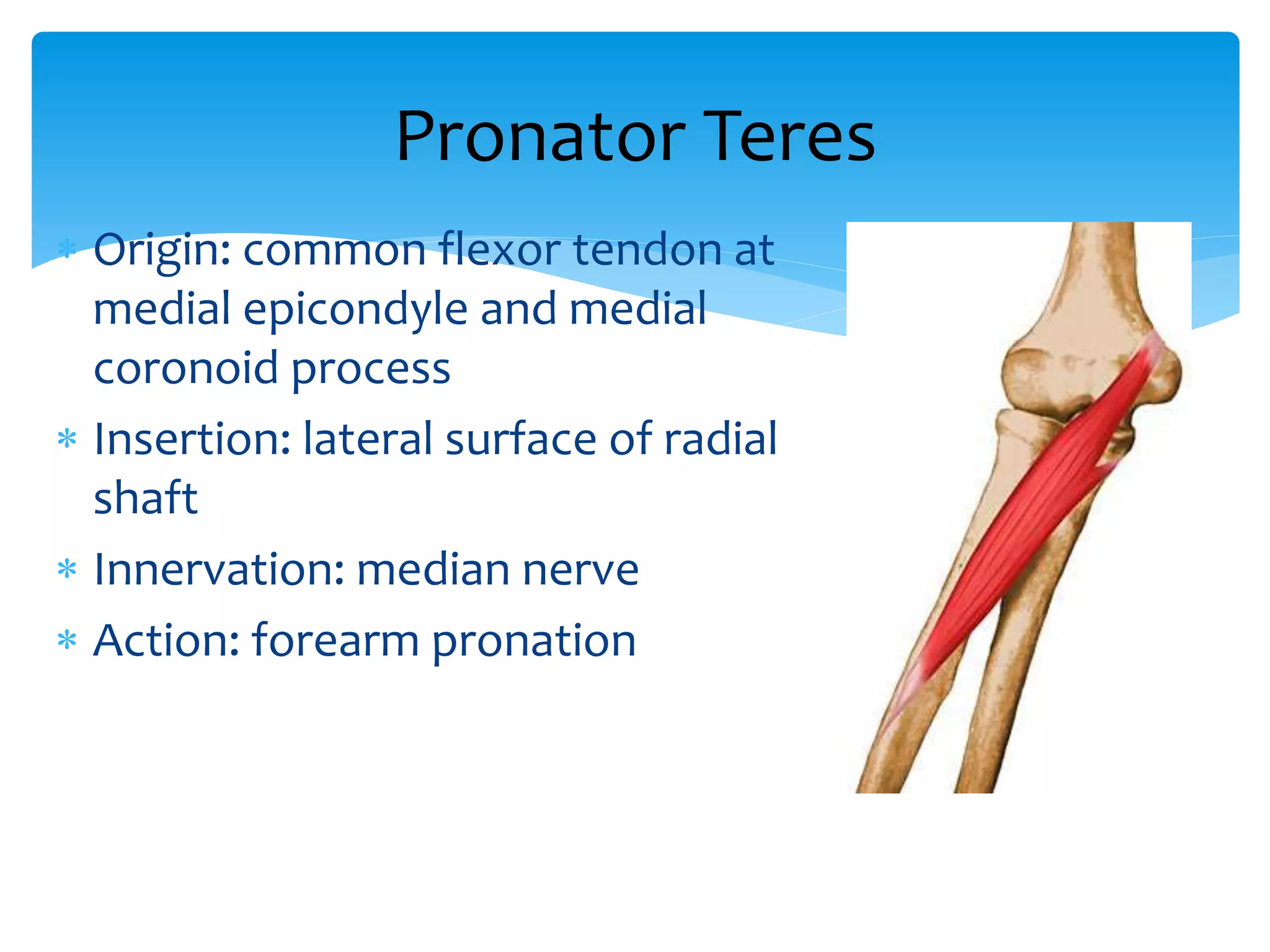
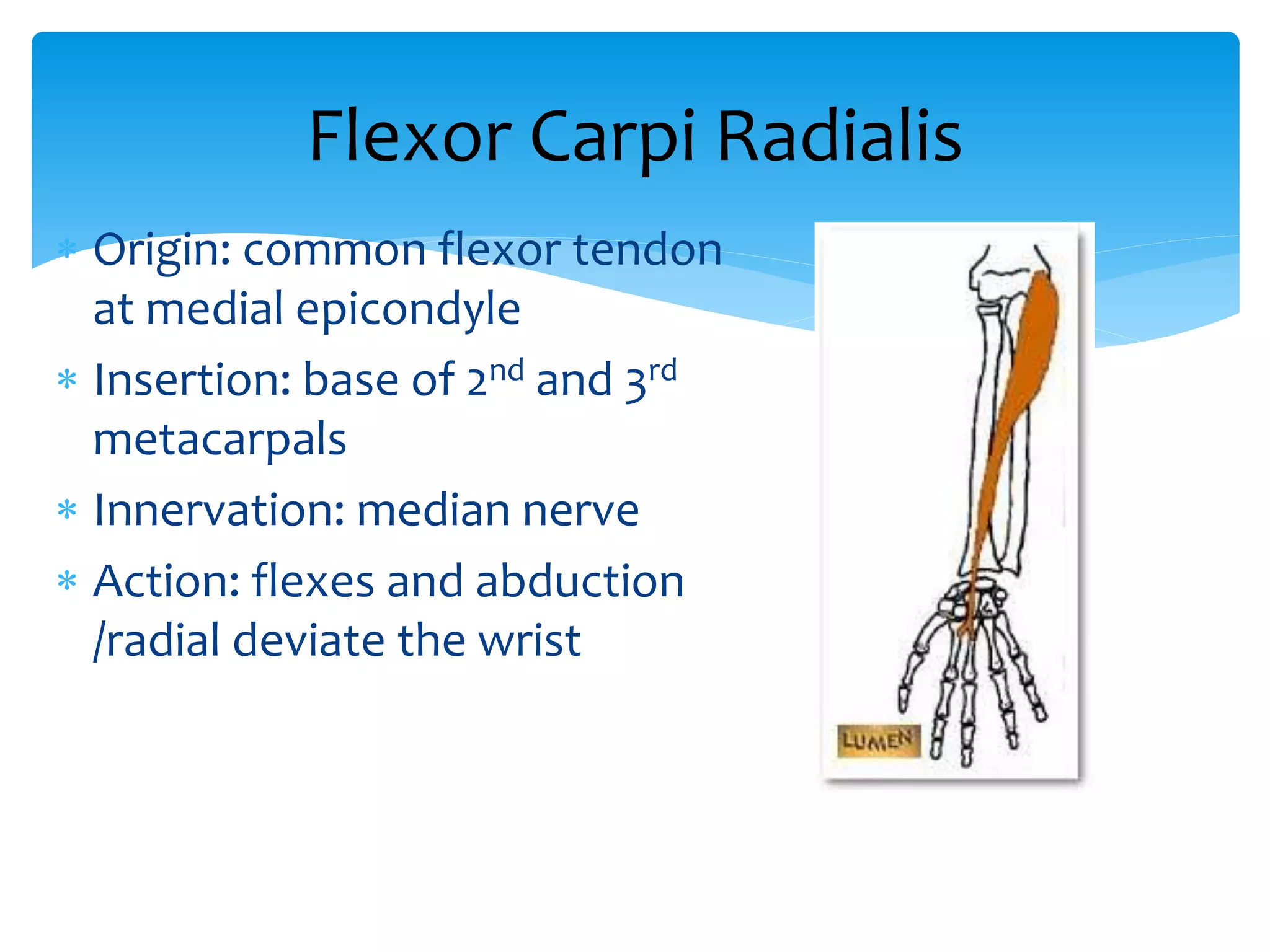
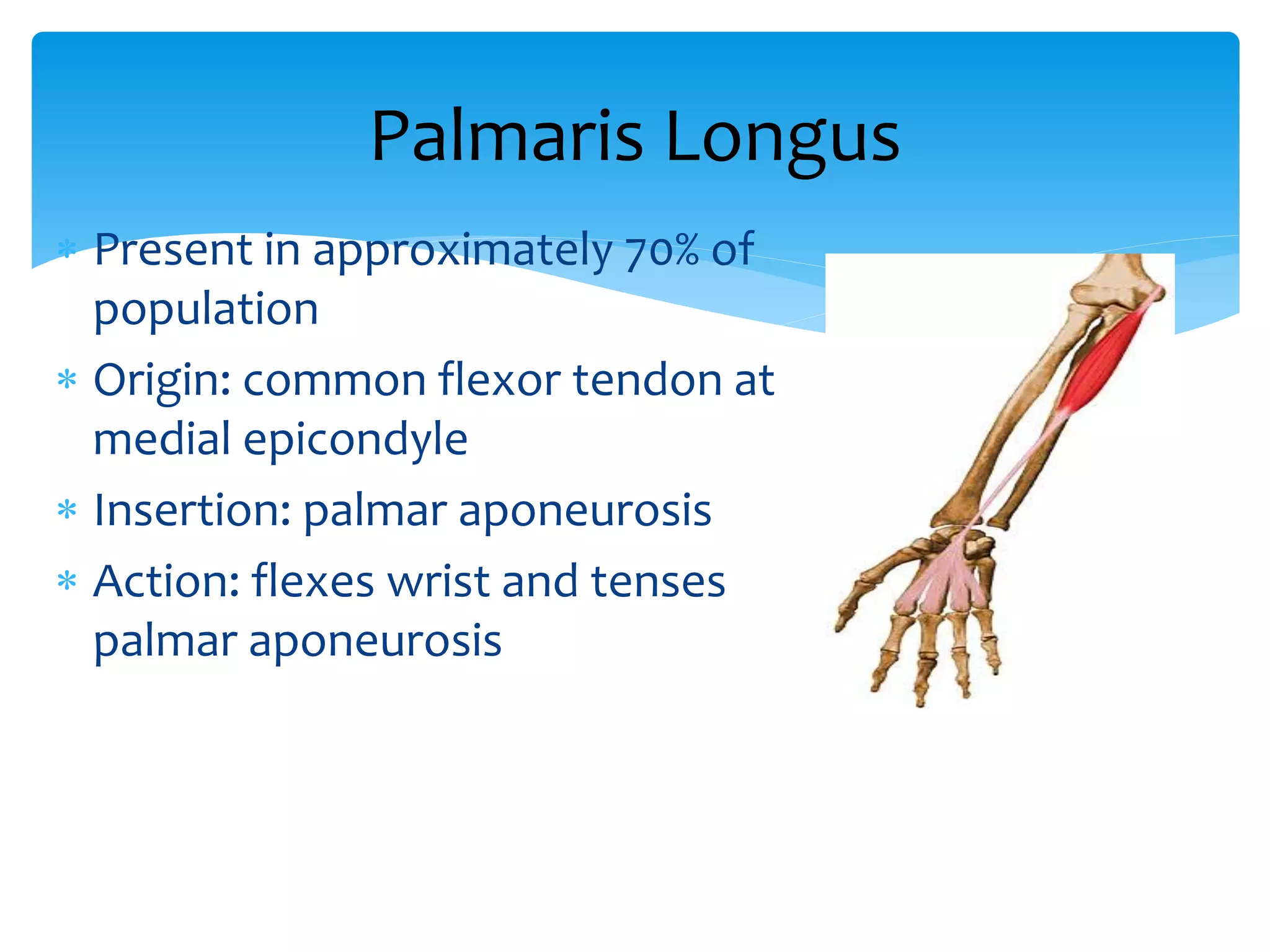
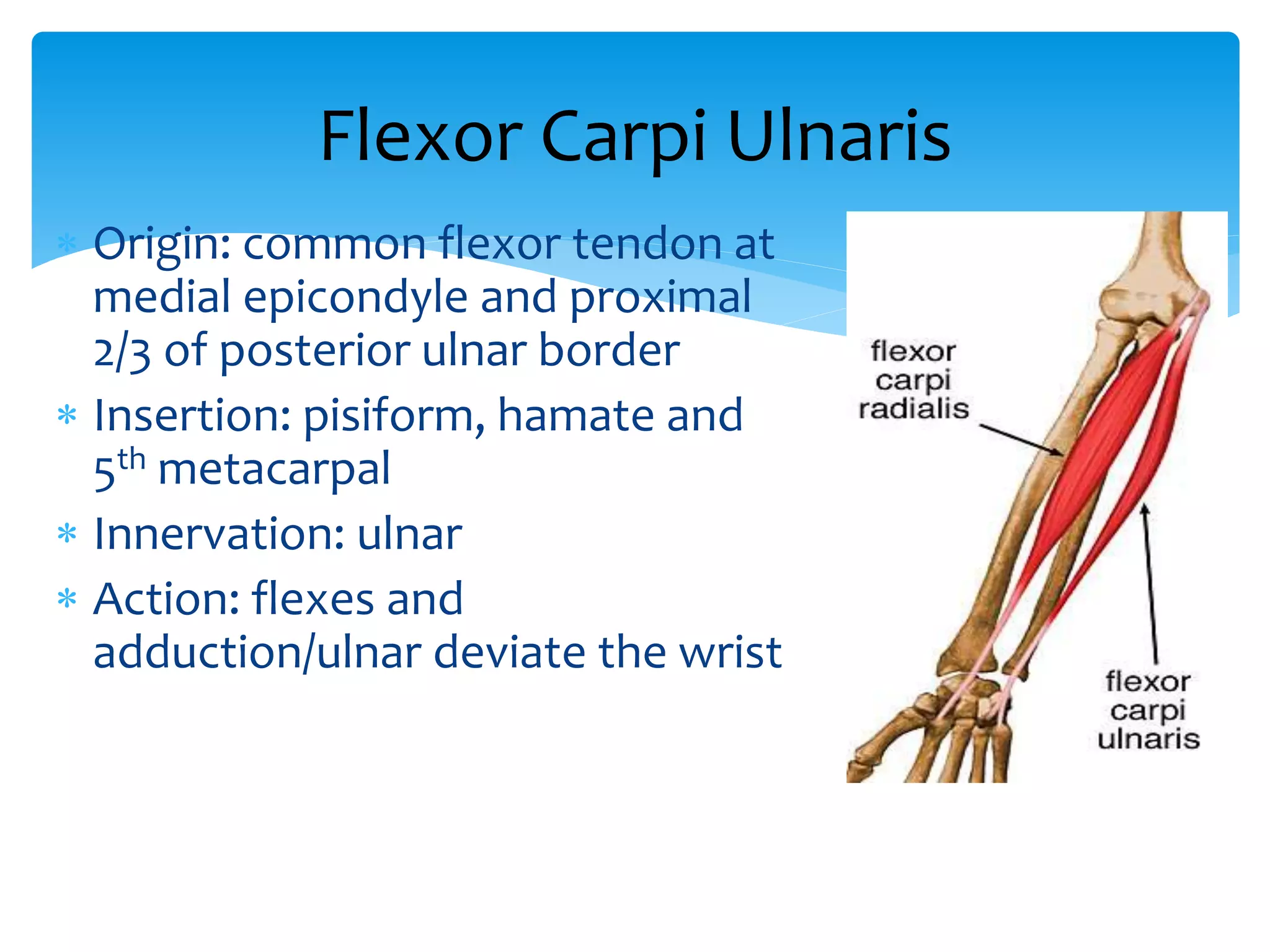
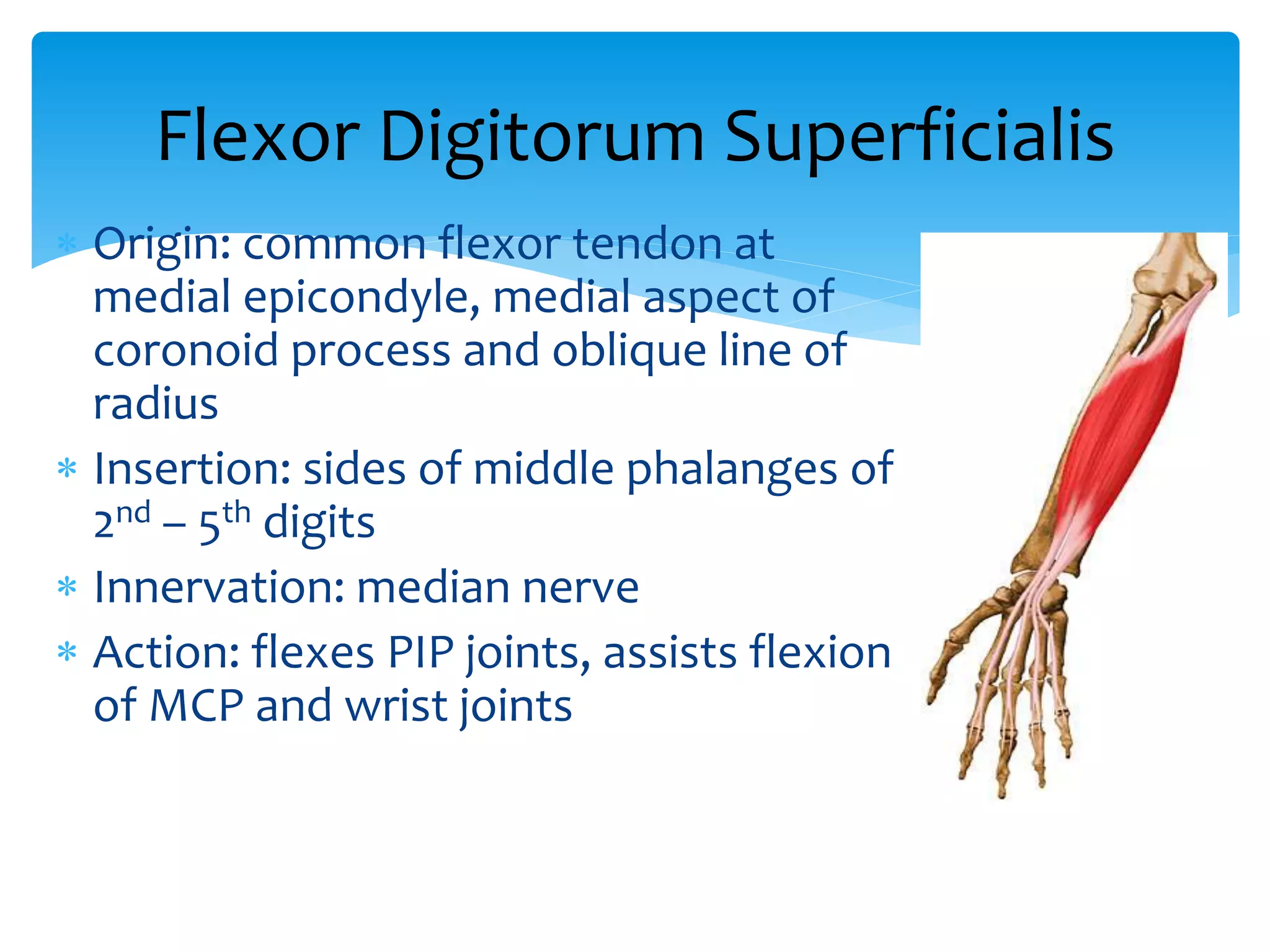
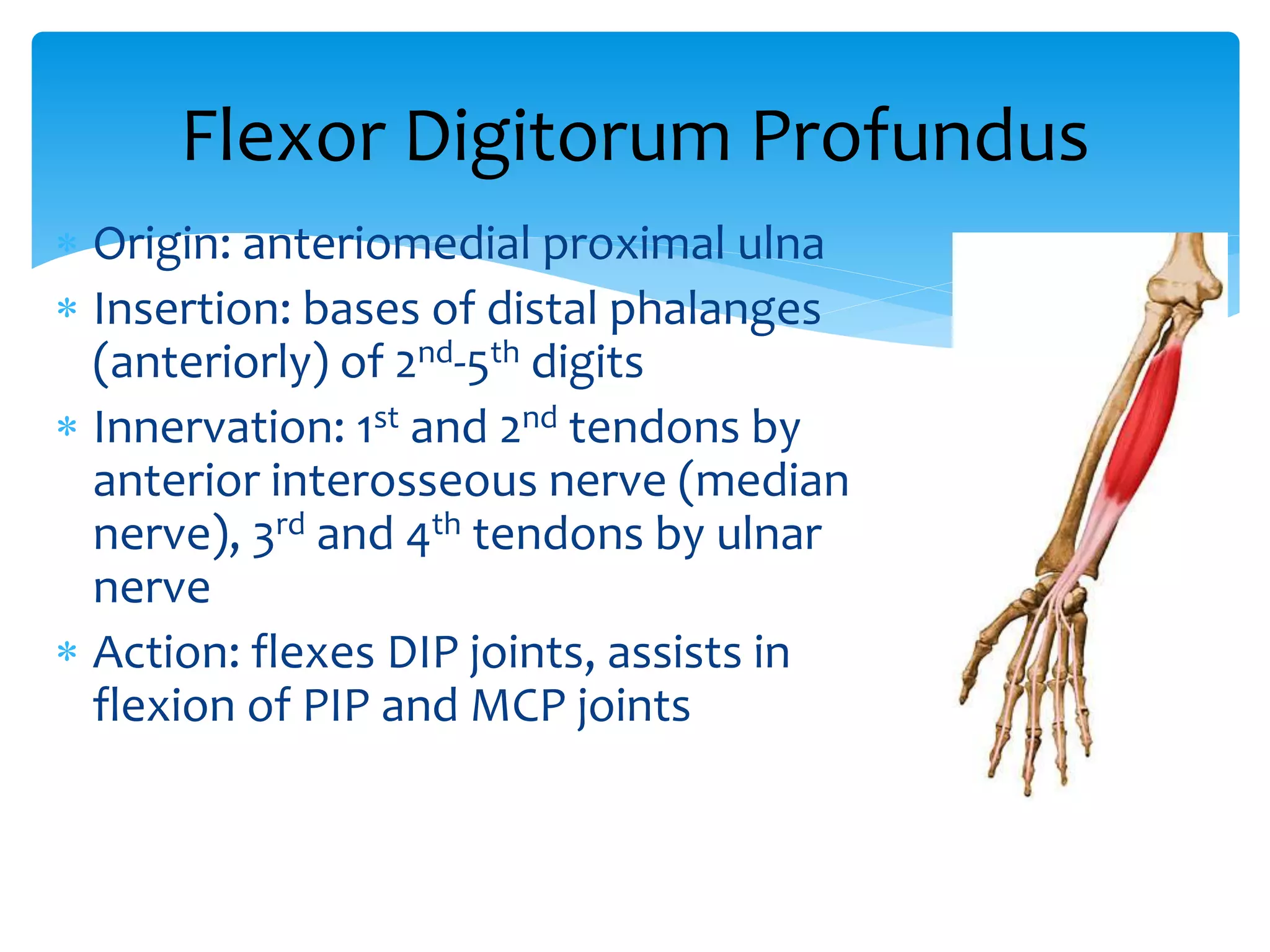
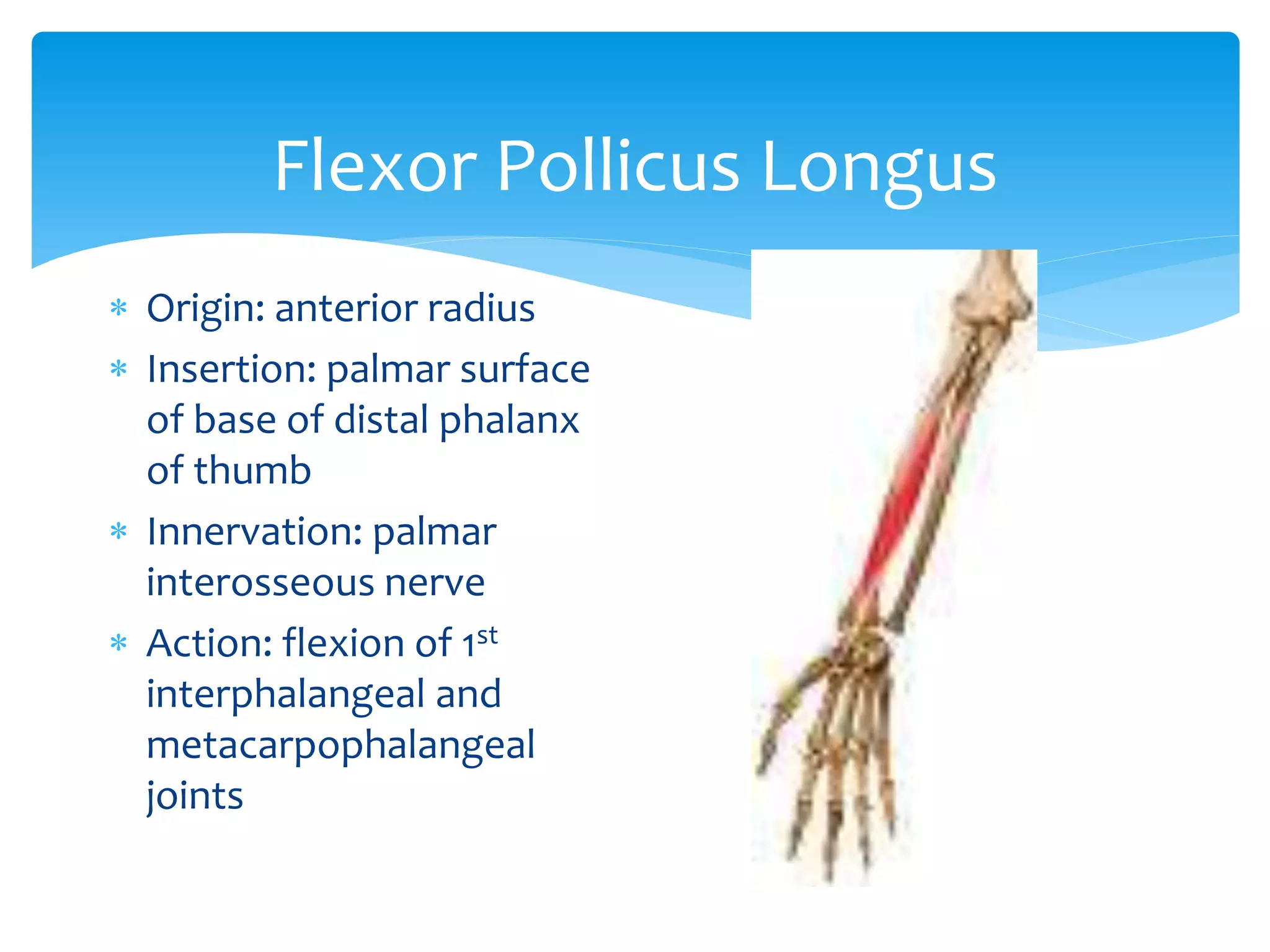
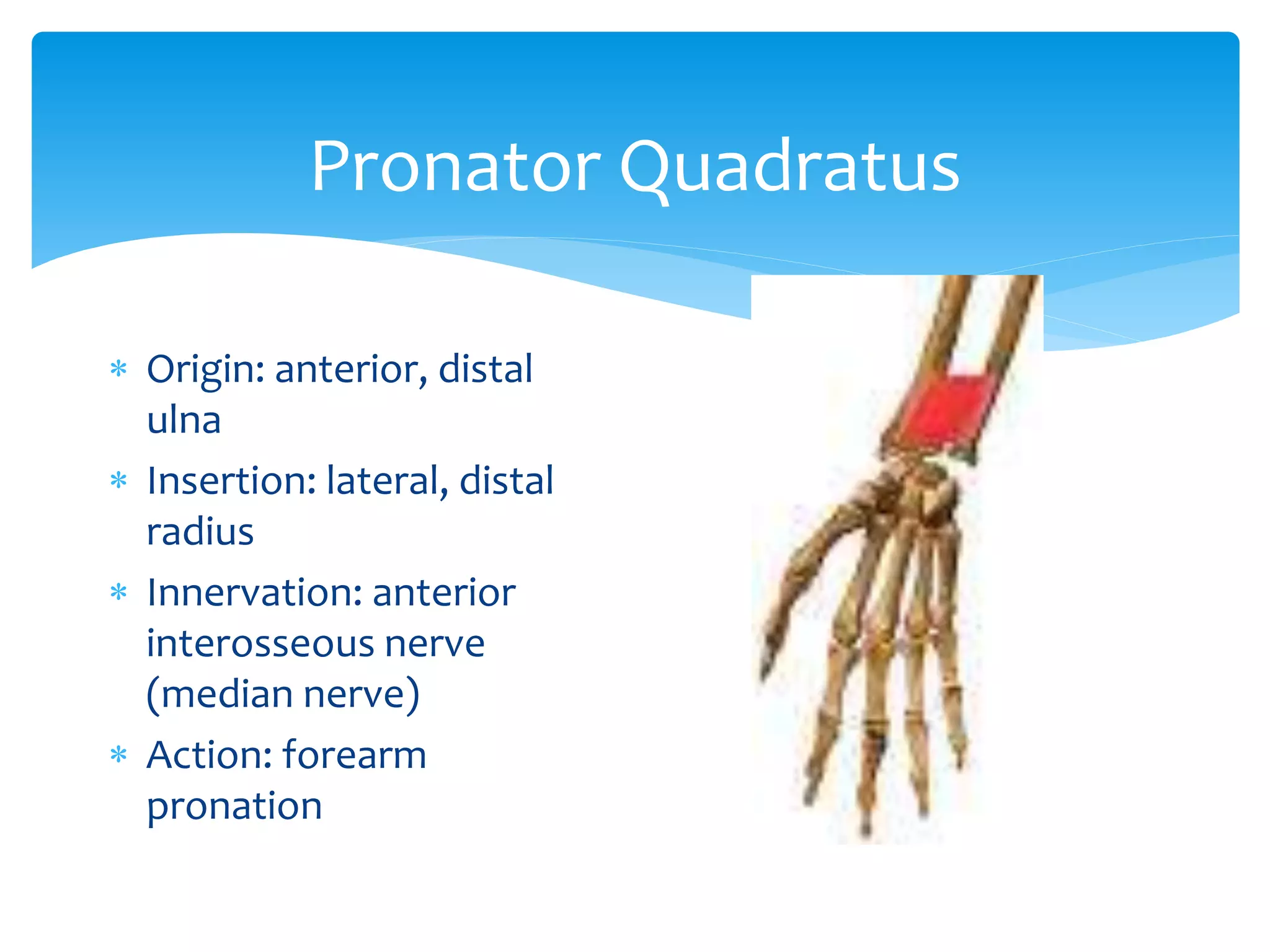
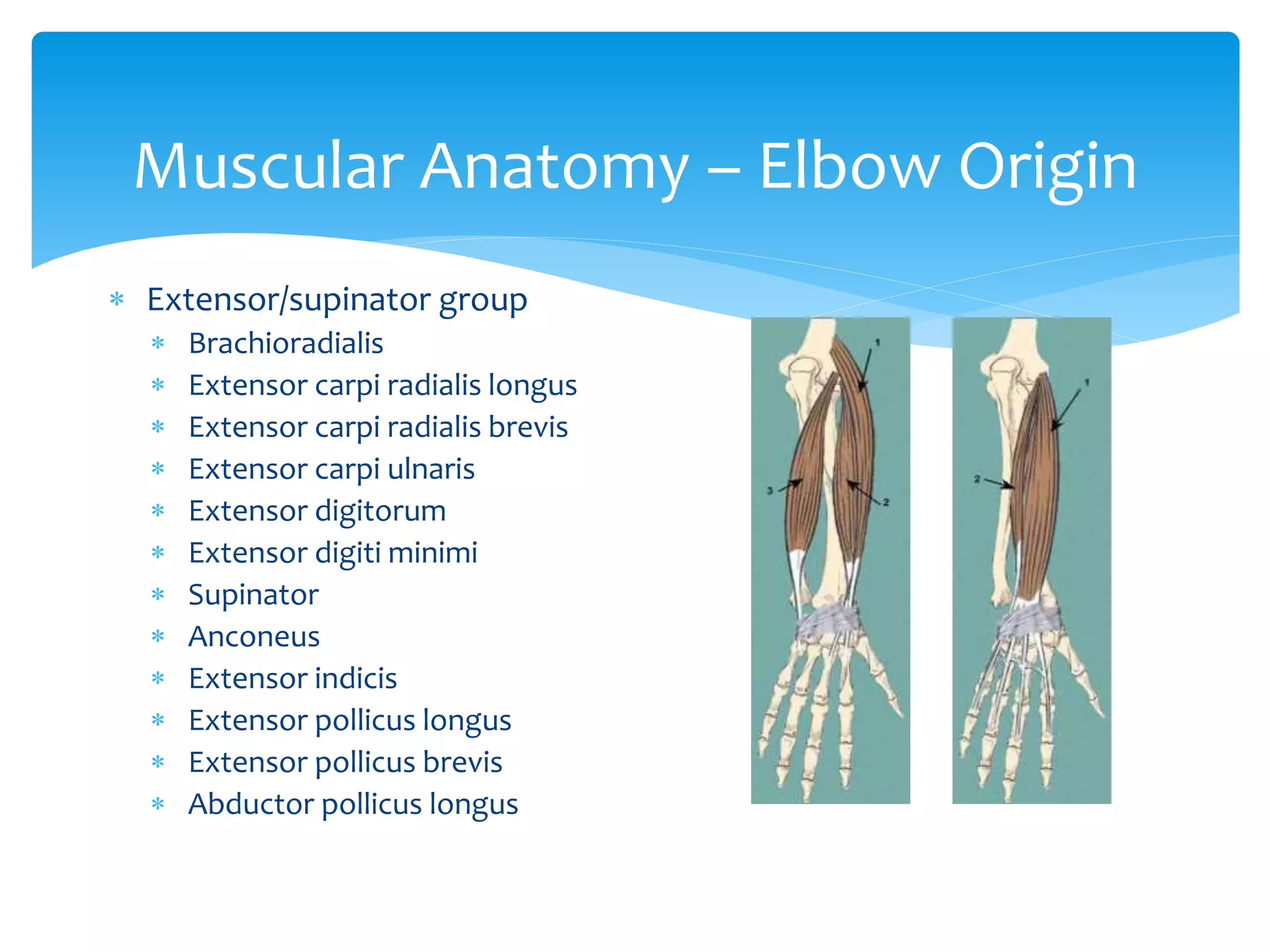
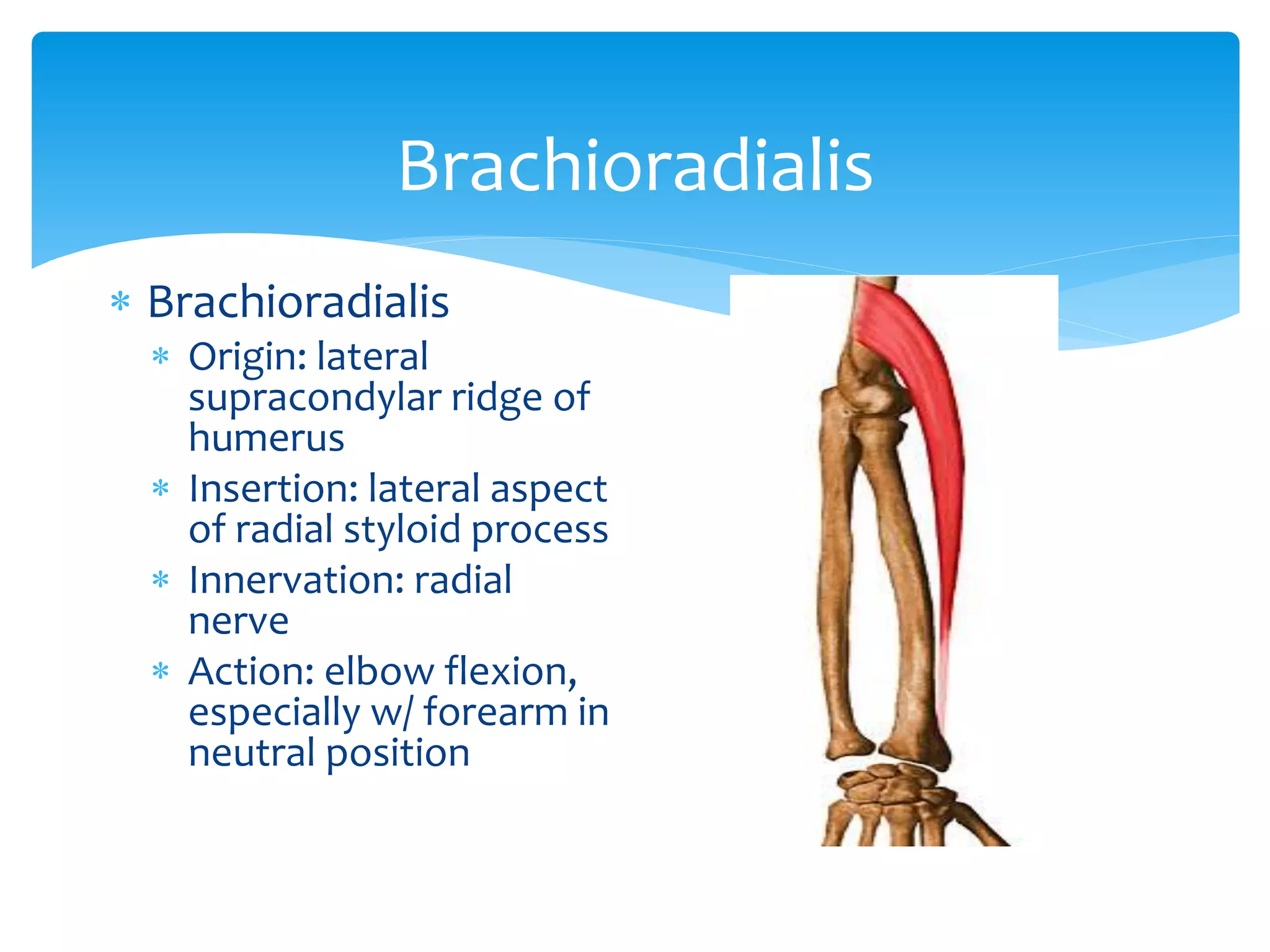
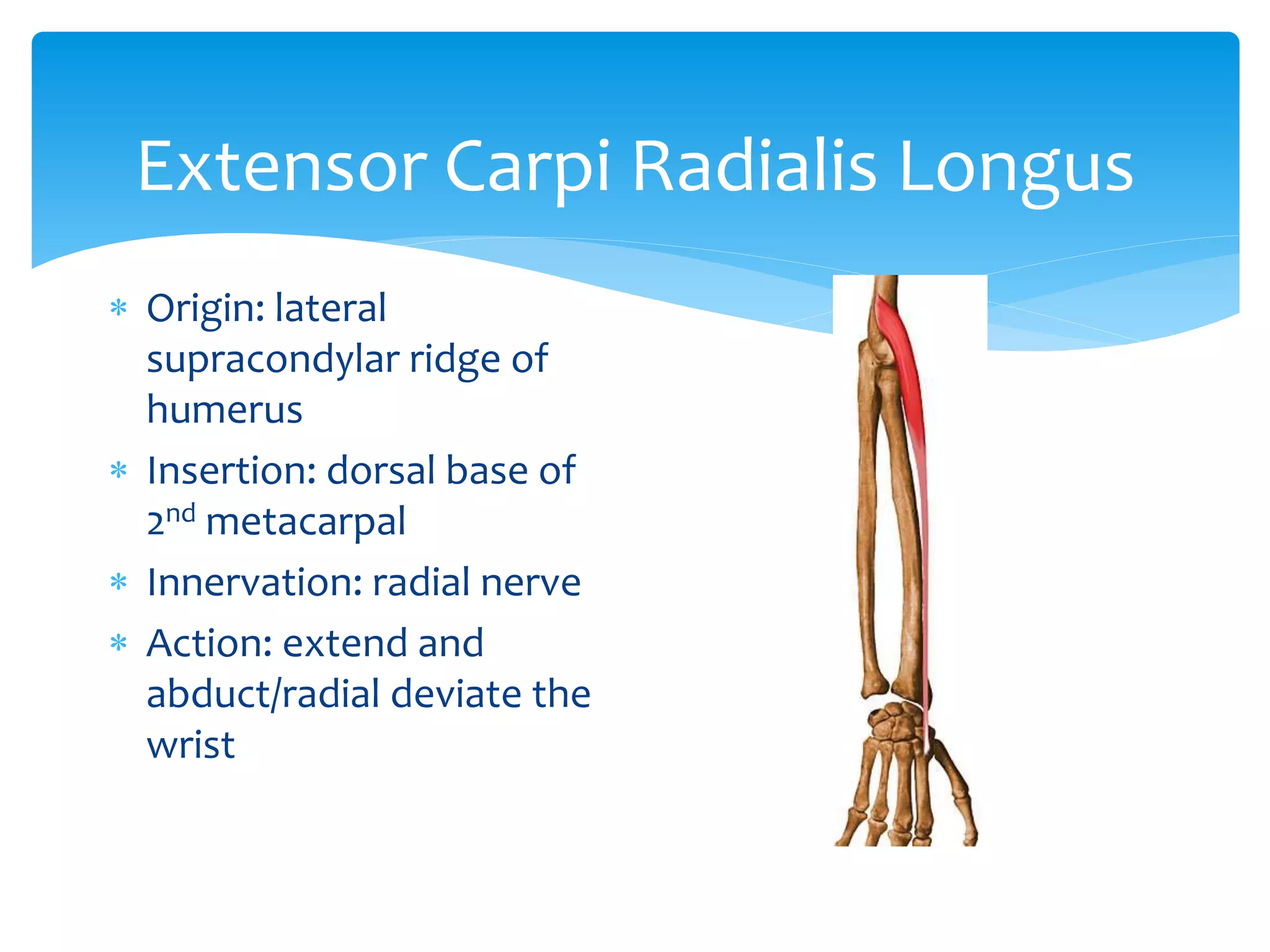
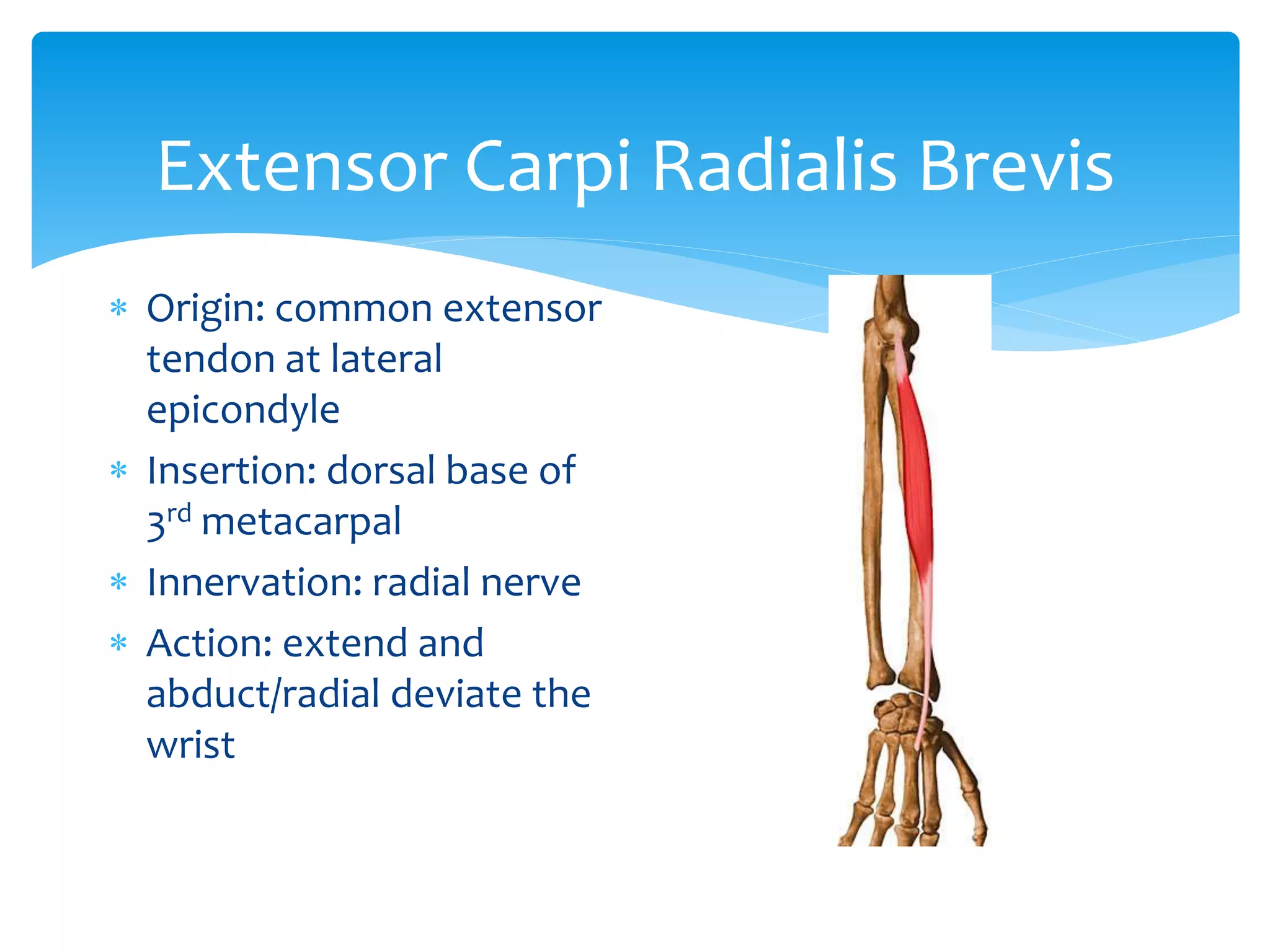
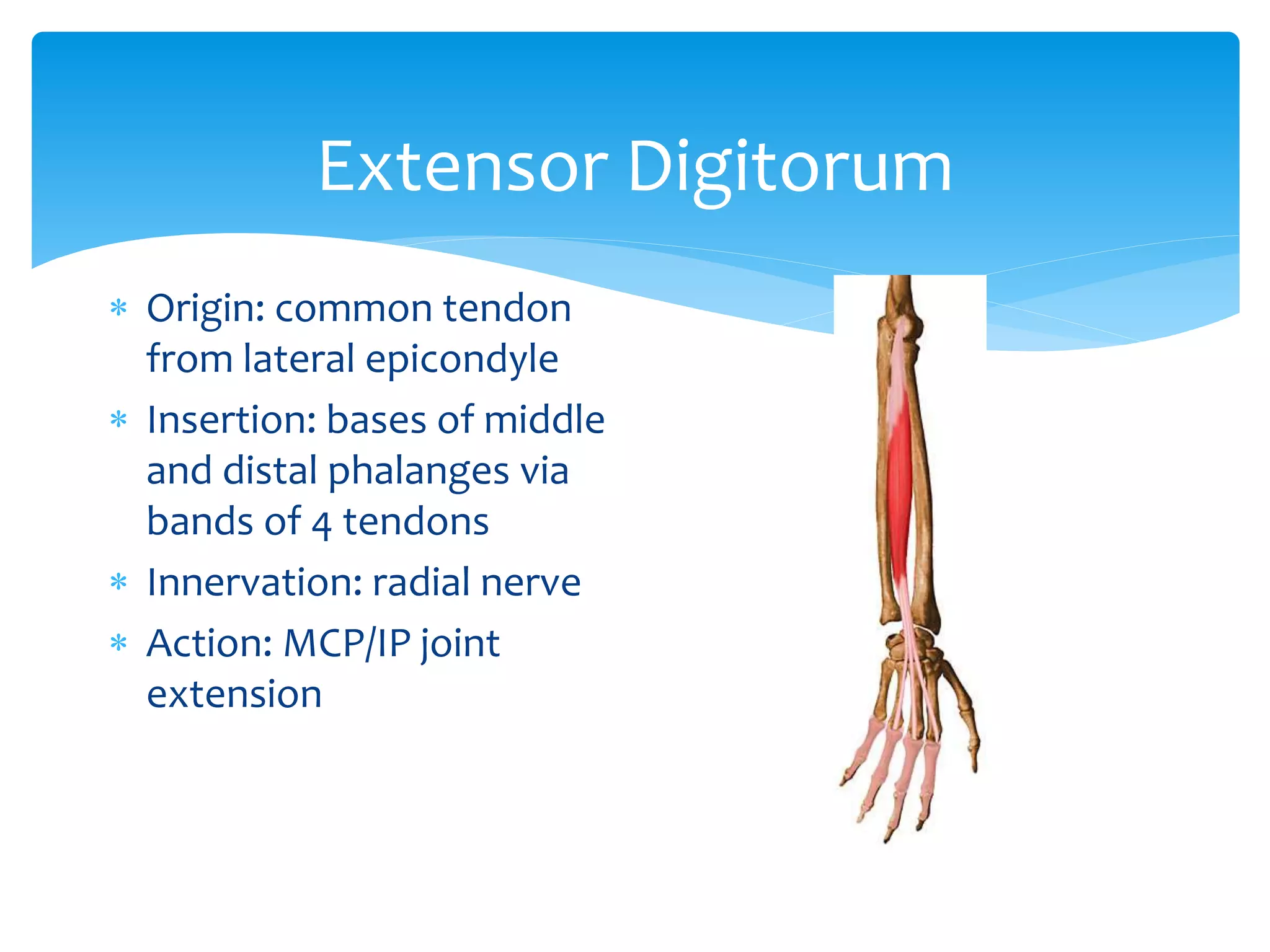
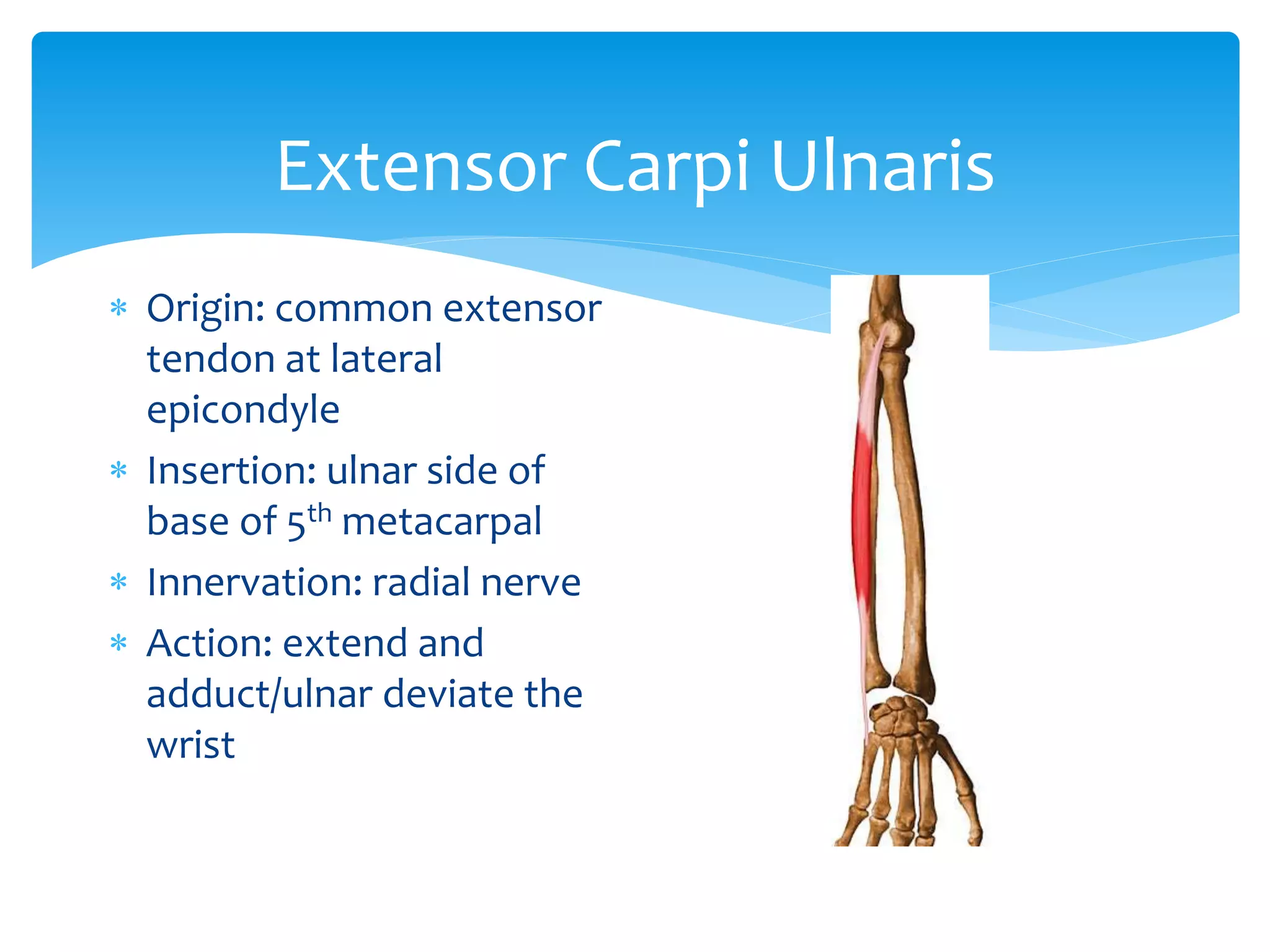
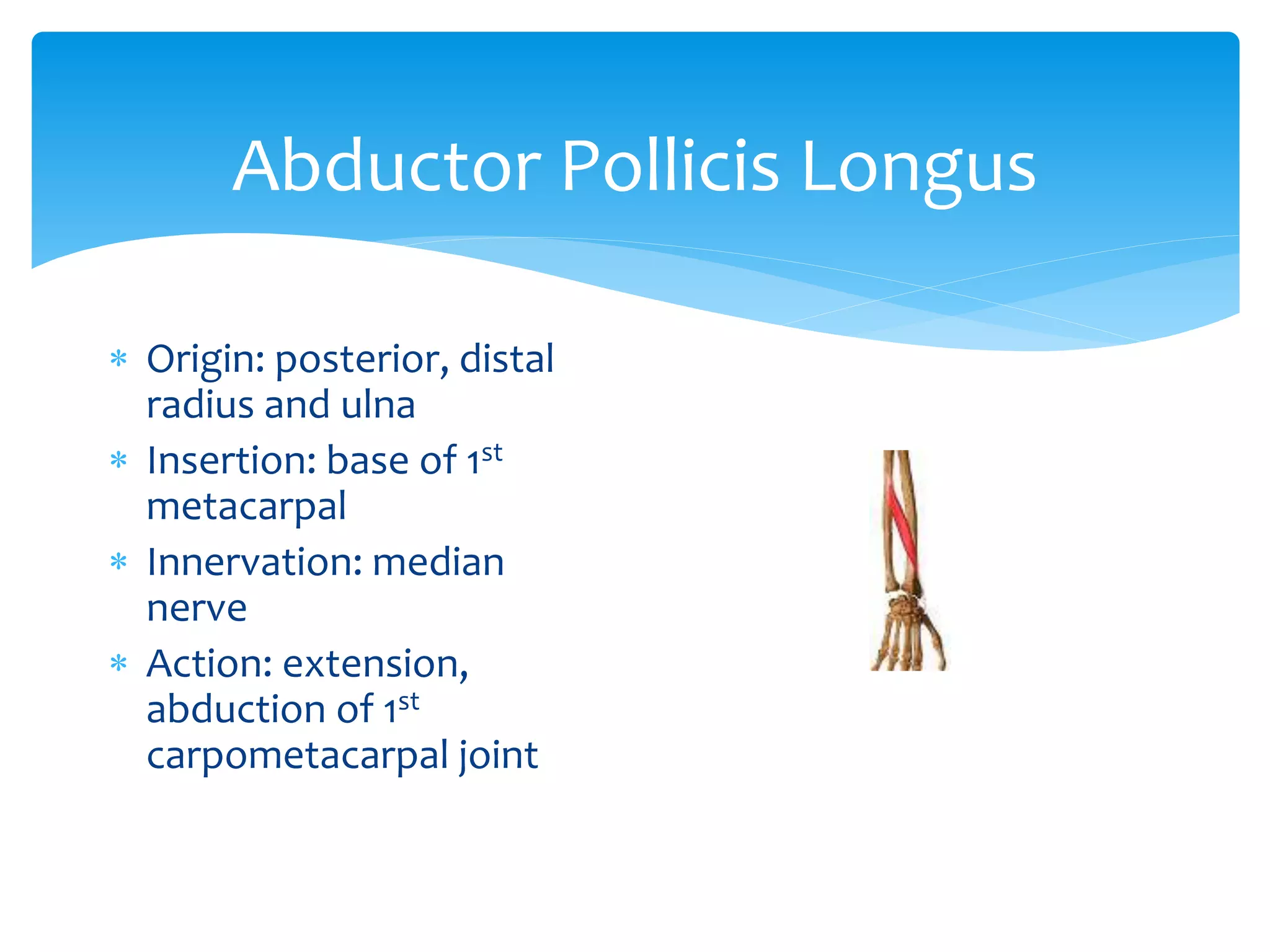
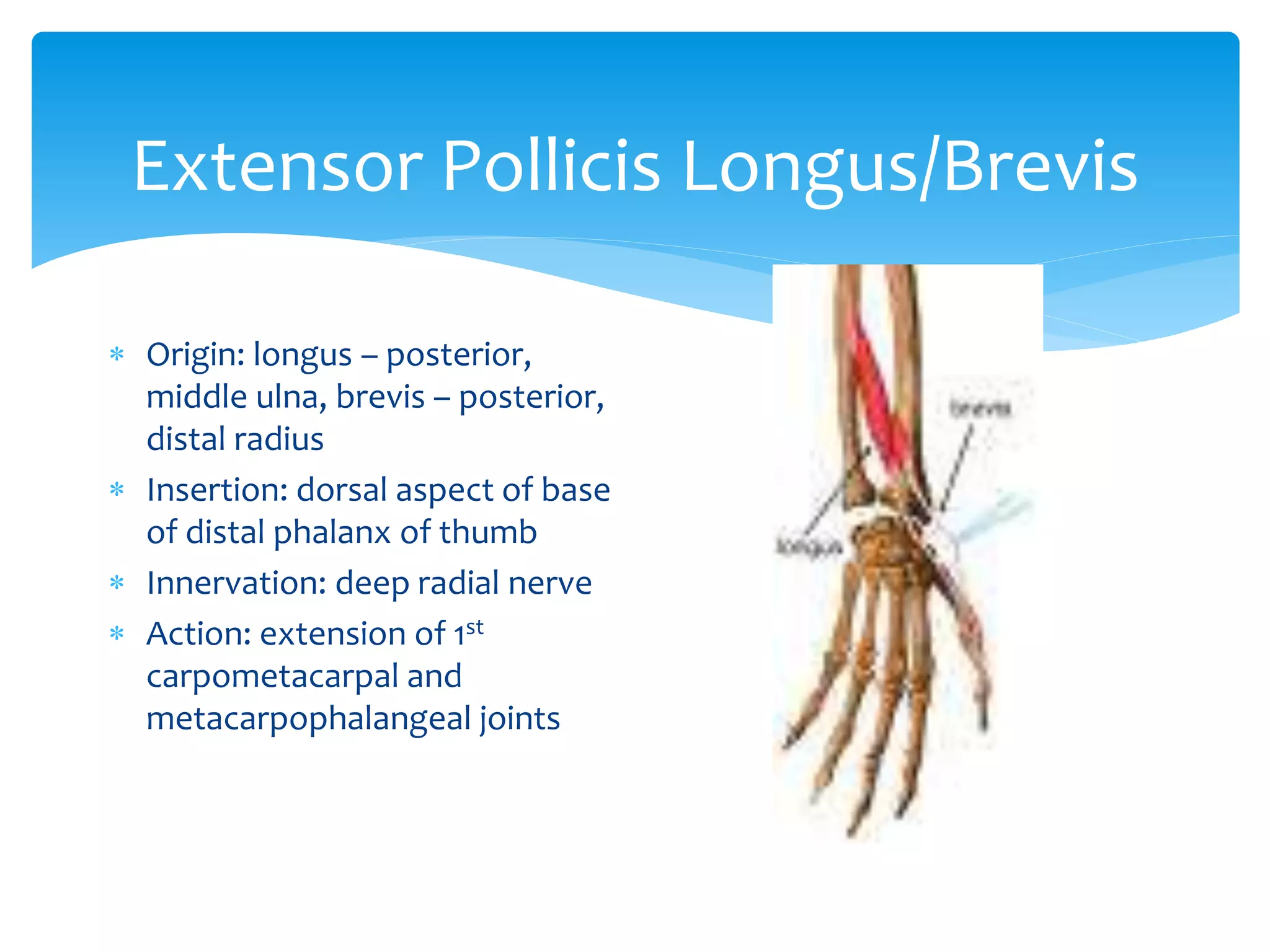
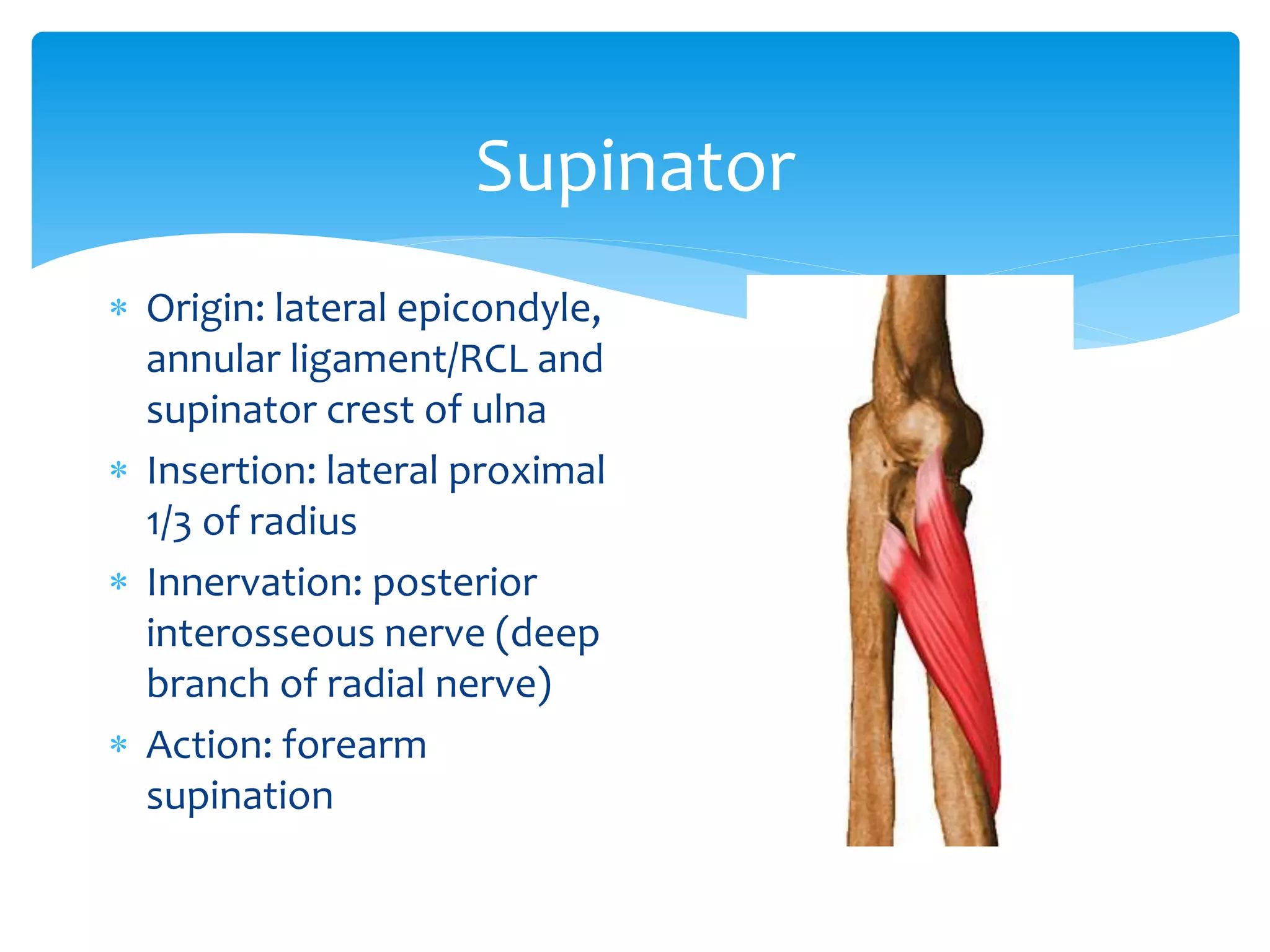
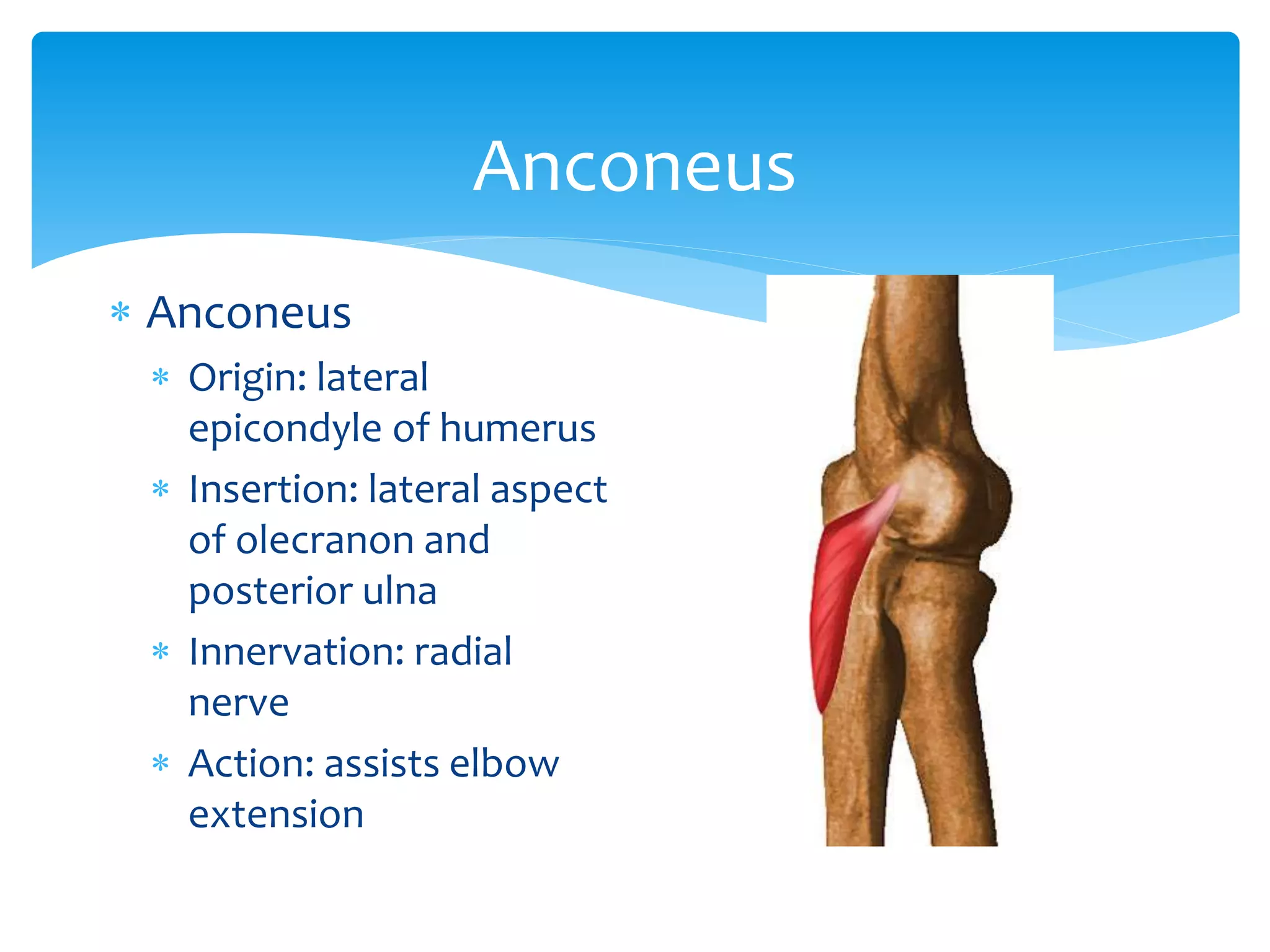
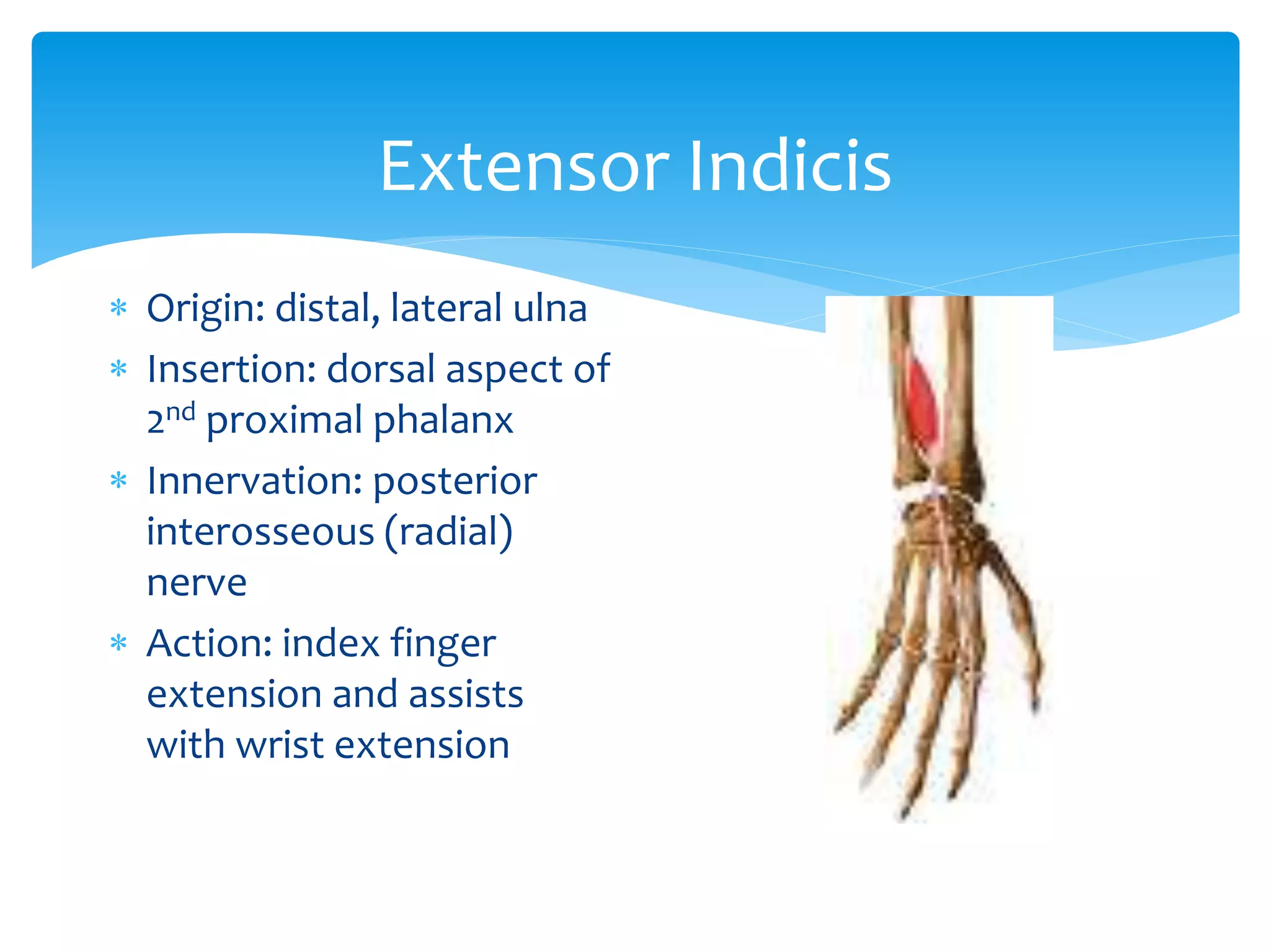
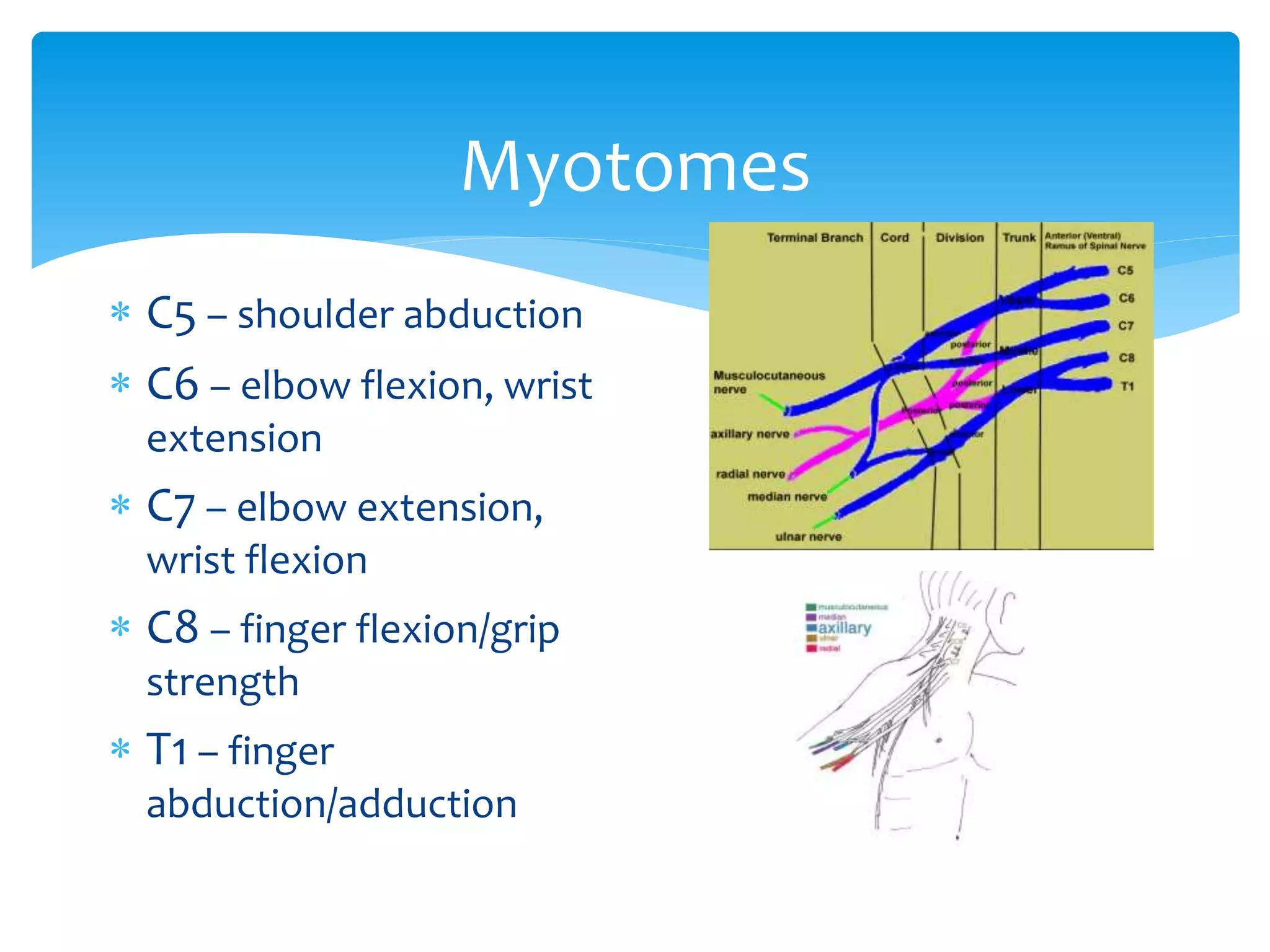
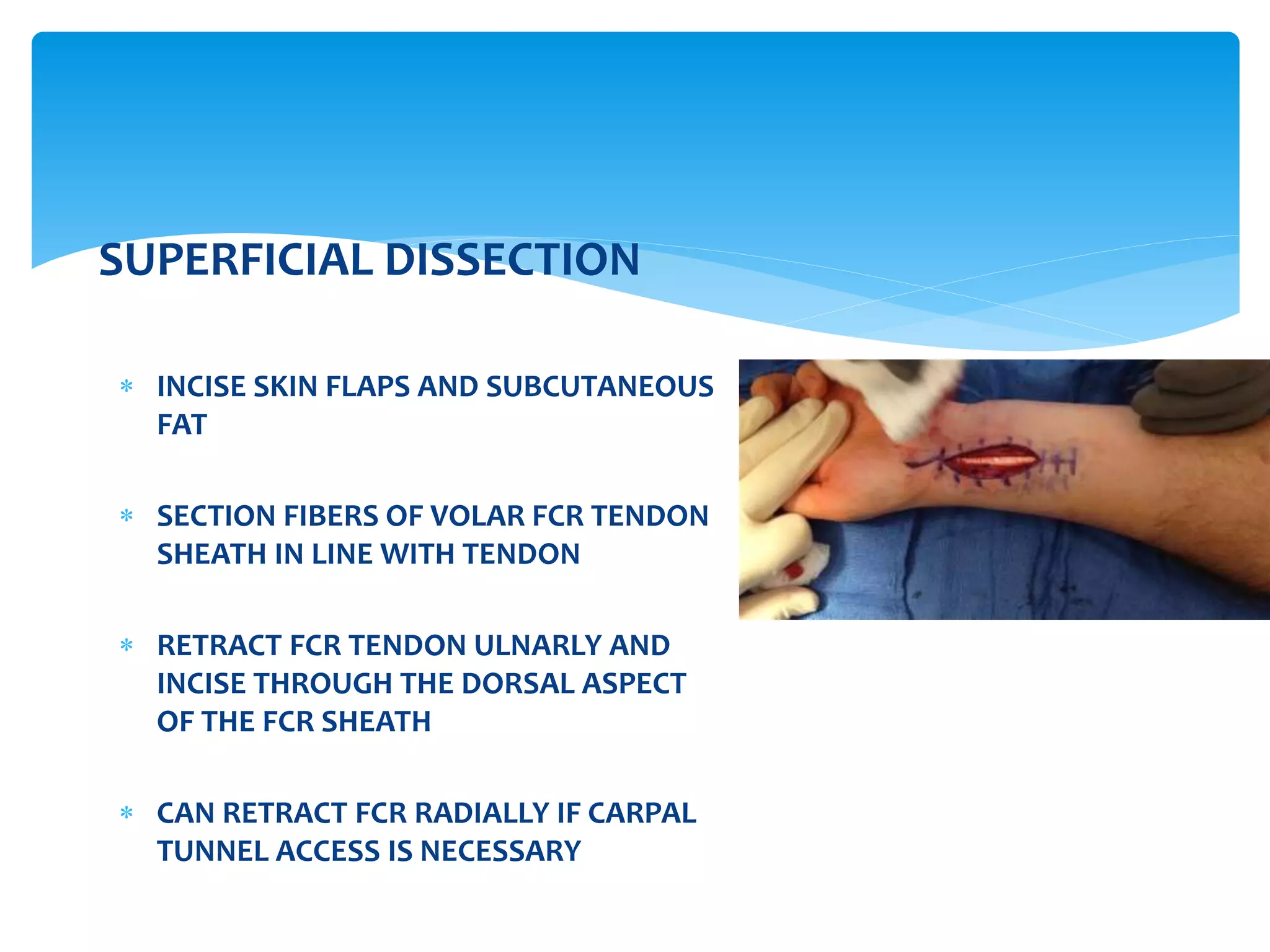
- Flexor and extensor muscle groups originate on the humerus, ulna, and radius to flex/extend the elbow, pronate/supinate the forearm, and flex/extend the wrist and fingers.
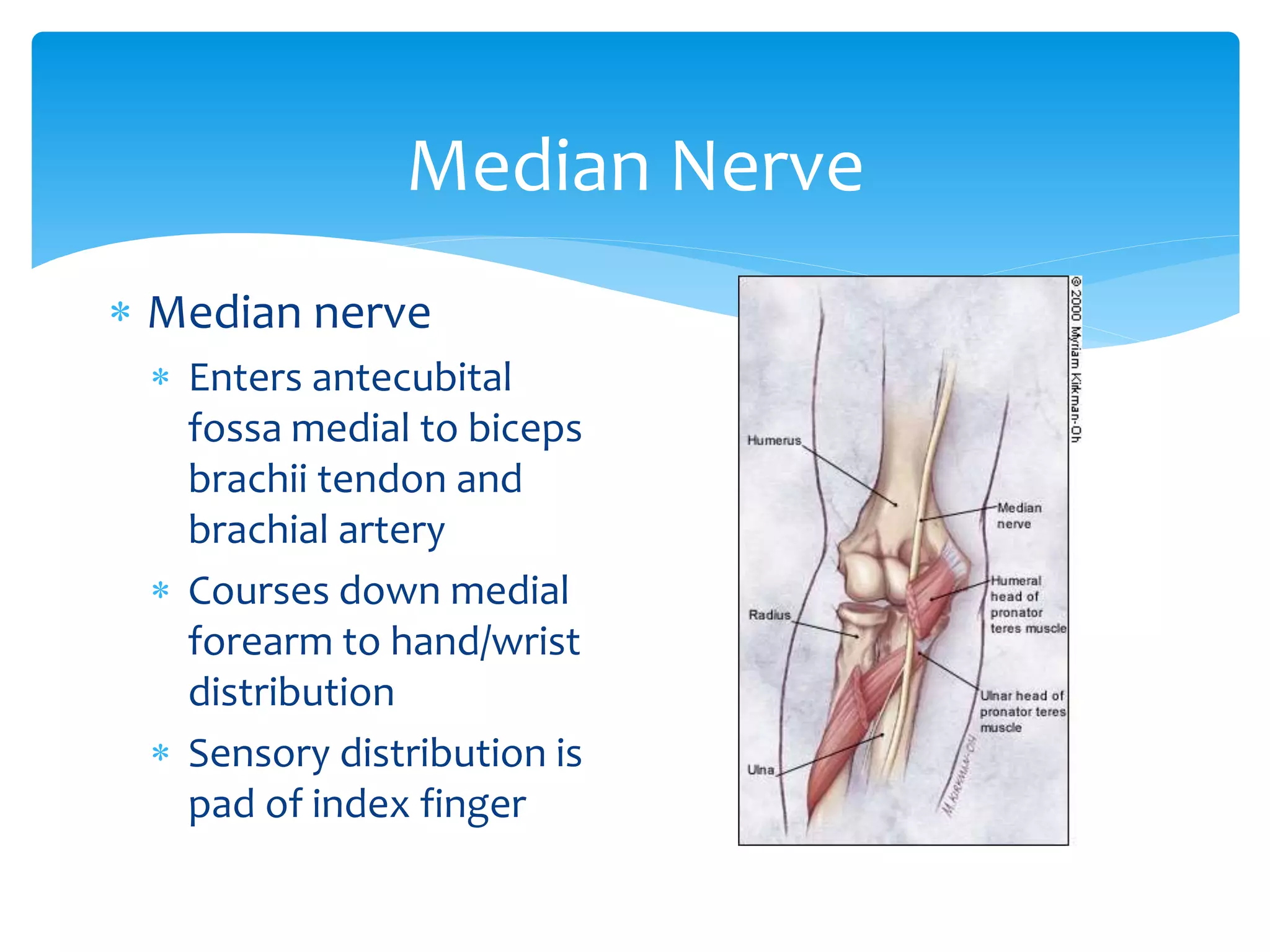
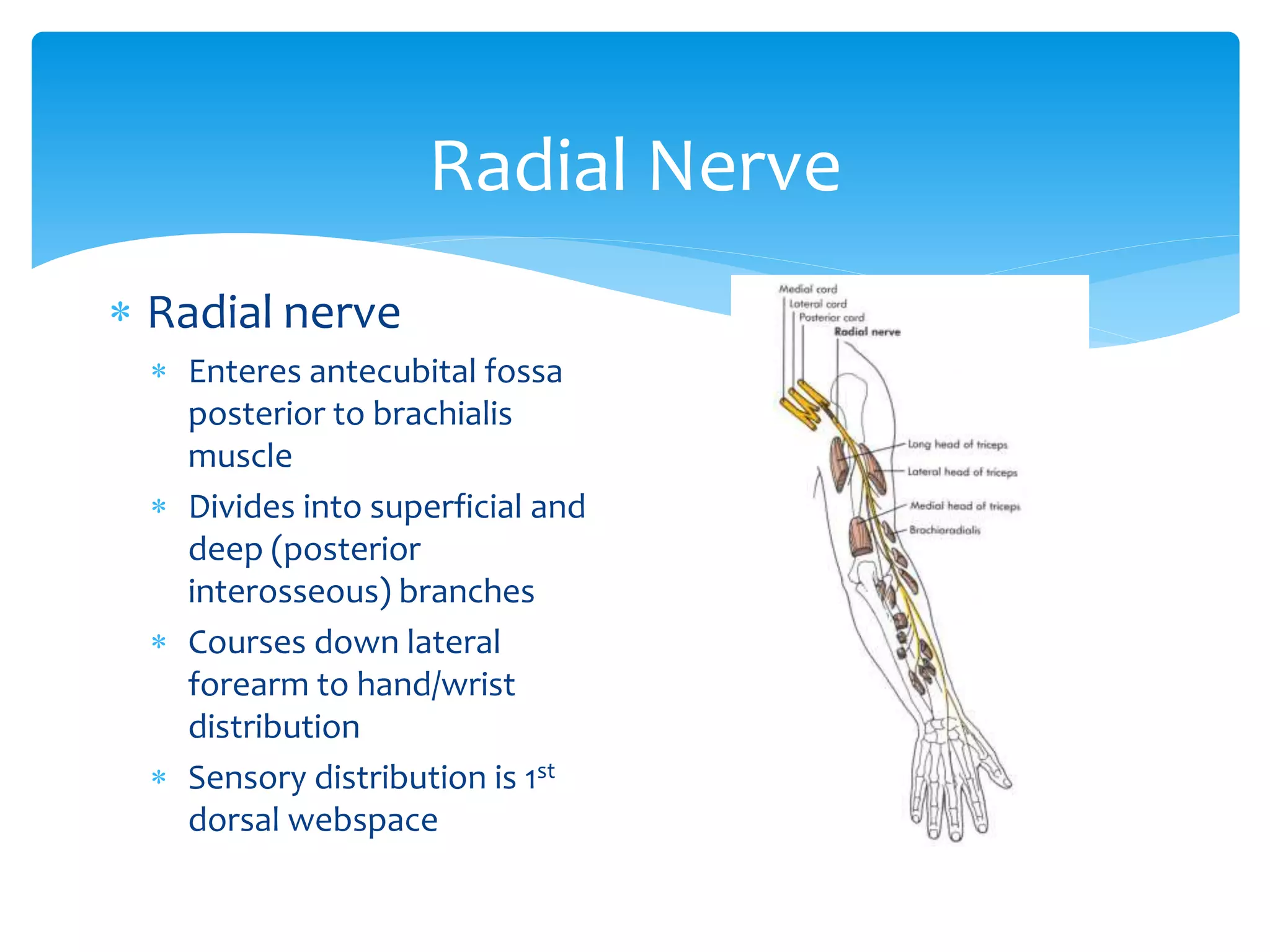
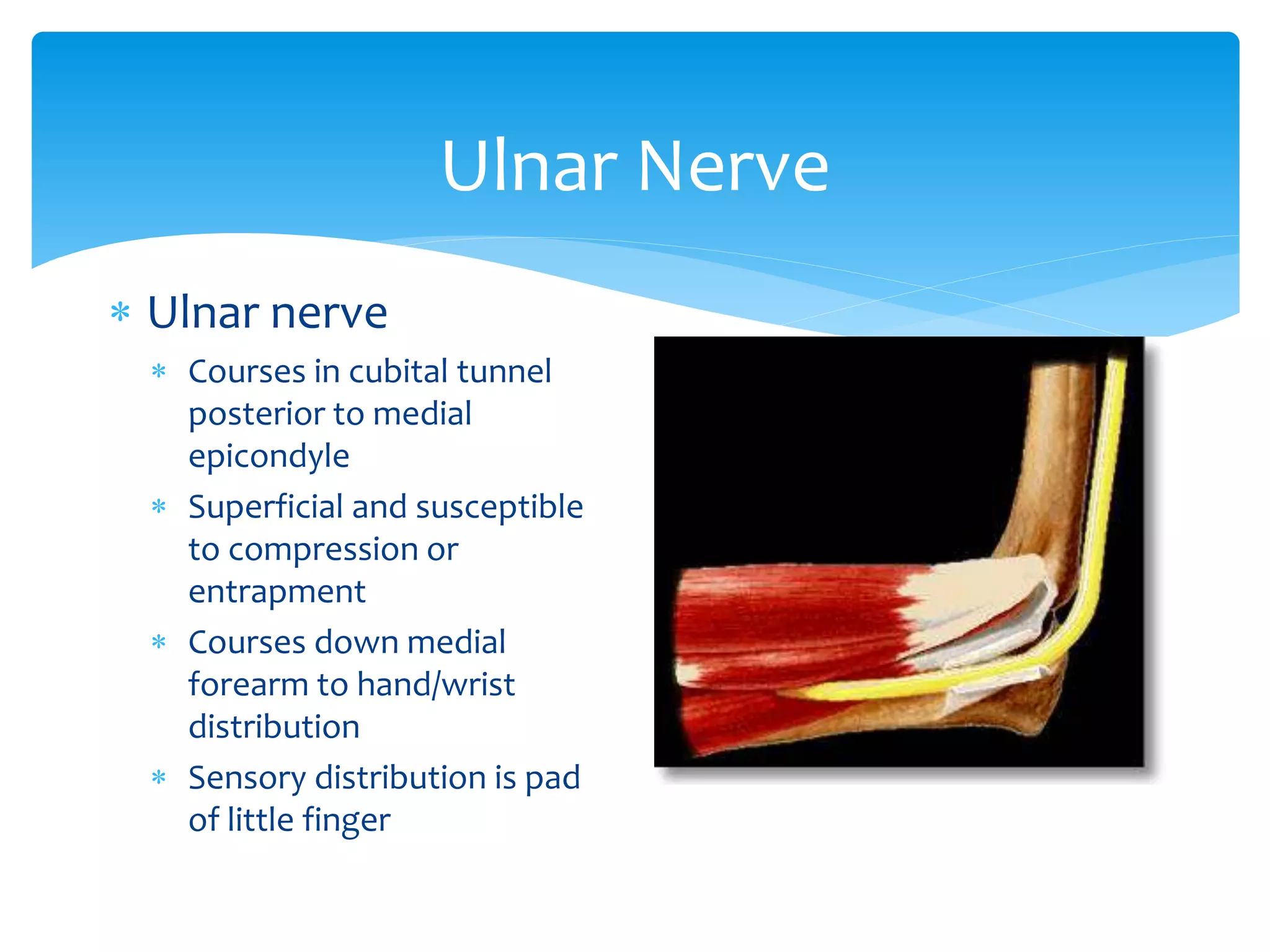
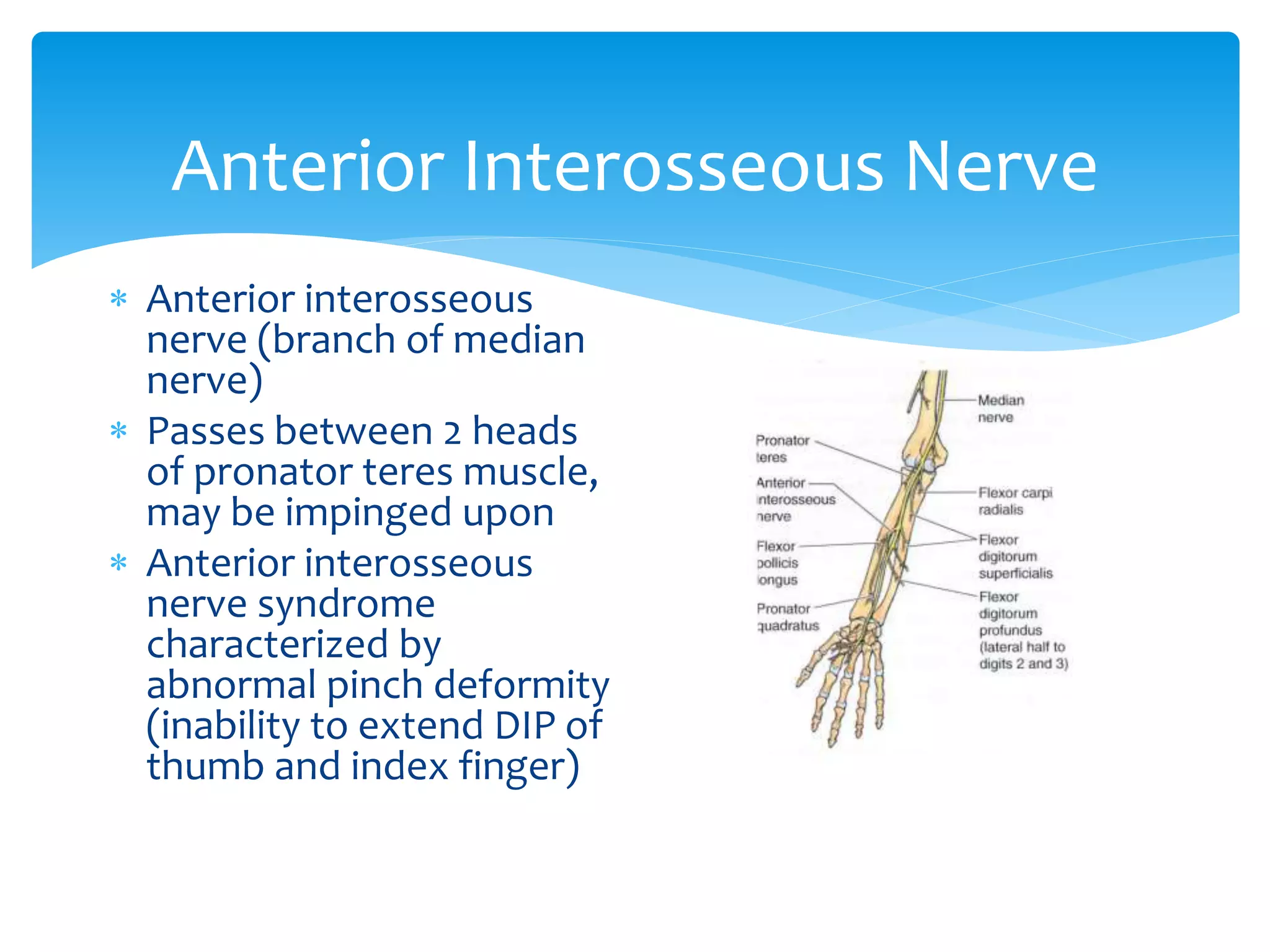
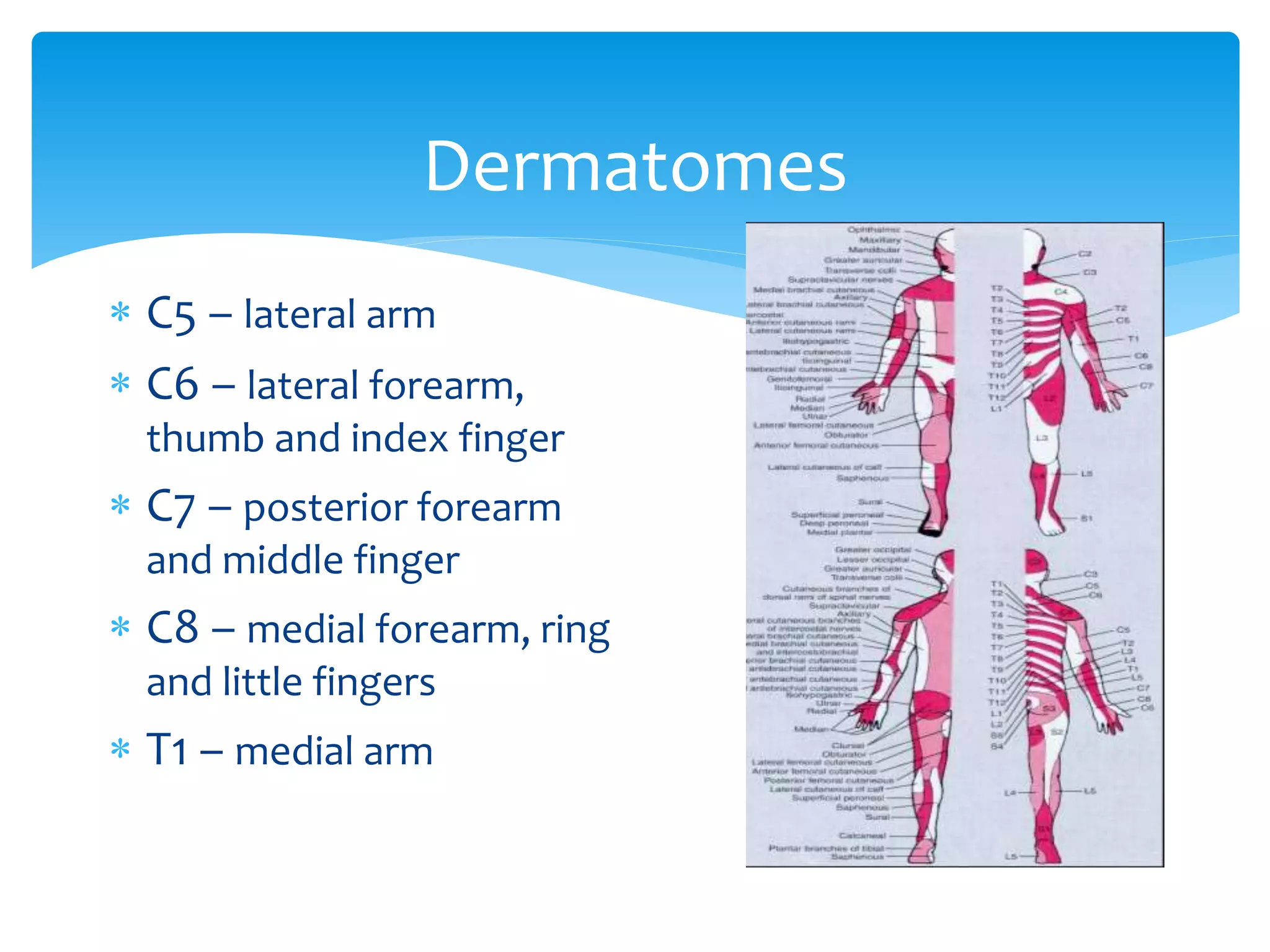
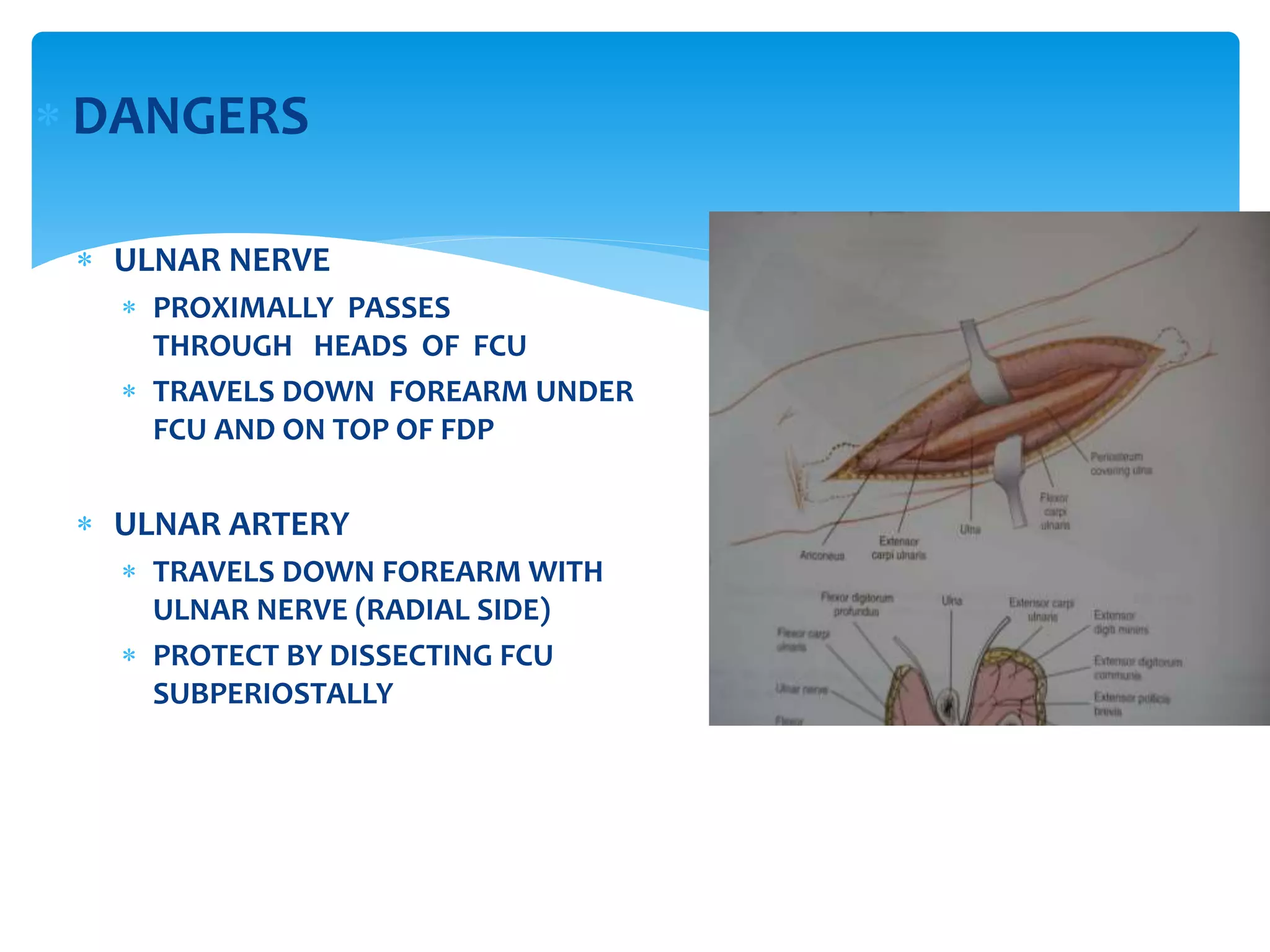
- The median, radial, and ulnar nerves innervate muscles in the forearm and hand.
-