Anatomy of ankle and foot
•
41 likes•1,751 views

Anatomy of Ankle and Foot describing ankle joint, sub talar joint, bones and muscles involved in ankle and foot, arches of foot

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Anatomy of ankle and foot
Similar to Anatomy of ankle and foot (20)
Recently uploaded
Recently uploaded (20)
Anatomy of ankle and foot
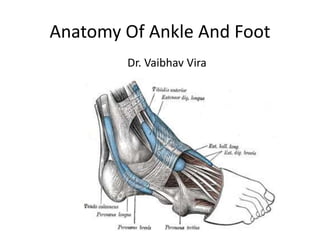
- 1. Anatomy Of Ankle And Foot Dr. Vaibhav Vira
- 2. Ankle • A/k/a talocrural joint • A diarthrodial articulation involving the distal tibia and fibula and the body of the talus • the only example in the human body of a true mortise joint
- 3. True Mortise
- 4. Foot • The human foot is a complex structure adapted to allow orthograde bipedal stance and locomotion and is the only part of the body that is in regular contact with the ground • There are 28 separate bones in the human foot, including the sesamoid bones of the first metatarsophalangeal joint, and 31 joints, including the ankle joint.
- 5. Foot (cont.) • Functionally, the skeleton of the foot may be divided into the tarsus, metatarsus and phalanges. • Anatomically it is divided into - • The hindfoot comprises the calcaneus and talus • The midfoot comprises the navicular, cuboid and three cuneiforms • The forefoot comprises five metatarsals, fourteen phalanges and two sesamoid bones of the great toe
- 6. Bones
- 7. Distal Tibia • The distal end of the tibia has 5 surfaces namely anterior, medial, posterior, lateral and distal surfaces, and projects inferomedially as the medial malleolus • The distal surface, also called the tibial plafond, articulates with the talus and is wider anteriorly than posteriorly • The medial malleolus is short and thick, and has a smooth lateral surface with a crescentic or comma-shaped facet that articulates with the medial surface of the talar body
- 8. Distal Fibula • The distal end of the fibula or lateral malleolus projects distally and posteriorly relative to the medial malleolus • Its lateral aspect is subcutaneous, the posterior surface has a broad groove with a prominent lateral border, and the anterior surface is rough and somewhat rounded and articulates with the anteroinferior aspect of the tibia. • The medial surface has a triangular articular facet and is vertically convex with its apex directed distally. It articulates with the lateral talar surface. Behind the facet is a rough malleolar fossa for ligamentous attachment
- 11. Tarsus • The seven tarsal bones occupy the proximal half of the foot • The tarsus and carpus are homologous, but the tarsal elements are larger, reflecting their role in supporting and distributing body weight. • The proximal row is made up of the talus and calcaneus • The distal row contains, from medial to lateral, the medial, intermediate and lateral cuneiforms and the cuboid.
- 12. • Medially, there is an additional single intermediate tarsal element, the navicular. • Collectively, these bones display an arched transverse alignment that is dorsally convex. Medially, the navicular is interposed between the head of the talus and the cuneiforms. Laterally, the calcaneus articulates with the cuboid. • The tarsus and metatarsus are arranged to form intersecting longitudinal and transverse arches. Hence, thrust and weight are not transmitted from the tibia to the ground (or vice versa) directly through the tarsus, but are distributed through the tarsals and metatarsals to the ends of the longitudinal arches.
- 13. Foot Bones
- 14. Talus • The talus is an intercalated bone with no tendinous attachments. It is the osseous link between the foot and leg through the ankle joint. It is the second largest tarsal bone • It Has Head, Neck And Body • Head:- Directed distally and somewhat inferomedially, the head has a distal surface, which is ovoid and convex; its long axis is also inclined inferomedially to articulate with the proximal navicular surface. • The Neck is the narrow, medially inclined region between the head and body. • The body is cuboidal in shape, superior (trochlear) surface articulates with tibia, inferior surface articulates with calcaneum, medial surface articulates superiorly with medial malleolus of tibia, lateral surface articulates with lateral malleolus of fibula, and small posterior surface
- 16. Calcaneus • In Latin Heel, forms prominence of heel • The calcaneus is the largest of the tarsal bones and projects posterior to the tibia and fibula as a short lever for muscles of the calf attached to its posterior surface. • It is irregularly cuboidal, its long axis directed forwards, upwards and laterally. • It has 6 surfaces namely, anterior, posterior, superior or dorsal, plantar, medial and lateral.
- 17. • Anterior surface is smallest surface and articulates with cuboid. • Posterior surface is where tendocalcaneus (tendo achillis) and plantaris is attached. • Superior surface is where it articulates with talus. • The plantar surface is rough and has three tubercles i.e. medial, lateral and anterior. Plantar ligament is attached on this surface. • Lateral surface is rough and flat • Medial surface is concave and have process called sustentaculum tali which assist in formation of talocalcaneonavicular joint
- 19. Navicular • Boat shaped • The navicular articulates with the talar head proximally and with the cuneiform bones distally. • 6 Surfaces namely anterior, posterior, superior or dorsal, plantar, medial and lateral. • Anterior surface articulates with three cuneiforms
- 21. Cuneiform Bones • Cuneiform = Wedge shaped • 3 Bones:- medial, intermediate and lateral • Medial is the largest and intermediate is smallest cunieform bone • Medial cuneiform has 6 surfaces • Intermediate cuneiform has 4 surfaces • Lateral cuneiform has 3 surfaces • Articulate with the navicular proximally and with the bases of the first to third metatarsals distally
- 22. Cuboid • The cuboid, the most lateral bone in the distal tarsal row, lies between the calcaneus proximally and the fourth and fifth metatarsals distally. • As name suggest it is cuboid, it has 6 surfaces namely anterior, posterior, superior (plantar) or dorsal, medial and lateral.
- 24. Metatarsus • Metatarsus is made up of 5 metatarsal bones numbered from medial to lateral. • Each metatarsal is miniature long bones having shaft, base and head. • Except for the first and fifth, the shafts are long and slender, longitudinally convex dorsally, and concave on their plantar aspects.
- 26. Phalanges • 28 phalanges • 14 in each foot • 2 in great toe and 3 for each of other toes
- 27. Soft Tissues Around Ankle Foot • Retinacula at the ankle:- Extensor Retinacula (Superior and Inferior), Flexor Retinaculum • Synovial Sheats at the Ankle • Plantar Aponeurosis • Fibular Retinacula (Superior And Inferior)
- 28. Extensor Retinacula • Deep fascia is thickened to form bands called retinaculum. • So called because they retain tendons in the place. • On front of the ankle there are extensor retinacula • Superior Extensor Retinaculum:- – Medially attached to the lower part of the anterior border of tibia – Laterally attached to the anterior boundary of the elongated triangular area just above lateral malleolus.
- 29. Extensor Retinaculum (cont.) • Inferior Extensor Retinaculum:- – Y shaped band of deep fascia, situated in front of the ankle joint and over posterior part of dorsum of the foot – Stem of Y is laterally, and upper and lower bands medially – Stem is attached to the anterior non articulating part of the superior surface of the calcaneum, in front of the sulcus calcanei – Upper band passes upwards and medially, and attaches to anterior border of medial malleolus – Inferior band passes downward and medially and attaches to the plantar aponeurosis
- 30. Extensor Retinaculum (cont.) • Structures passing under Superior and Inferior Extensor Retinaculum are (from Medial to Lateral):- – Tibialis Anterior – Extensor Hallucis Longus – Anterior Tibial Vessels – Deep Peroneal Nerve – Extensor Digitorum Longus – The Peroneus Tertius
- 32. Flexor Retinaculum (Tarsal Tunnel) • 2.5cm broad • Attachments:- – Anteriorly to the posterior border and tip of the medial malleolus – Posteriorly and laterally to the medial tubercle • Structures passing deep to retinaculum are (from medial to lateral): – The tendon of the tibialis posterior – The tendon of the flexor digitorum longus
- 33. – Posterior tibial artery and terminal branch with accompanying veins. – Tibial Nerve and its branches – Tendon of Flexor hallucis longus Lowest Part of the deep surface of retinaculum give origin to greater part of abductor hallucis muscle
- 34. Plantar Aponeurosis • It is the thickened central part of deep fascia • The plantar aponeurosis is composed of densely compacted collagen fibres orientated mainly longitudinally, but also transversely. • It represents distal part of plantaris which was seperated from rest of muscle during evolution. • It is triangular in shape with apex being proximal.
- 35. • Apex is attached to medial tubercle of the calcaneum, proximal to attachment of flexor digitorum brevis • Base is distal and divides into five processes near the head of the metatarsal bones. • Each process splits into superficial and deep slip. • Superficial slip is attached to skin • Deep slips embrace flexor tendons and blends with fibrous flexor sheet and deep transverse ligaments.
- 36. • It divides the sole into three compartments by septas • Function of Plantar Aponeurosis: – Fixes the skin to the sole – Protects the deeper structures – Helps in maintaining the longitudinal arches of the foot – Gives origin to muscles of the first layer of the sole
- 38. Synovial Sheats at Ankle • Anterior to the ankle, the synovial sheath for tibialis anterior extends from the proximal margin of the superior extensor retinaculum to the interval between the diverging limbs of the inferior retinaculum. • Posteromedial to the ankle, the sheath for tibialis posterior starts approximately 4 cm above the medial malleolus and ends just proximal to the attachment of the tendon to the tuberosity of the navicular • Posterolateral to the ankle, the tendons of fibularis longus and brevis are enclosed in a single sheath deep to the superior fibular retinaculum. This sheath splits into two separate sheaths enclosing their respective tendons deep to the inferior fibular retinaculum.
- 39. Fibular Retinacular • The fibular retinacula are fibrous bands that retain the tendons of fibularis longus and brevis in position as these tendons cross the lateral aspect of the ankle region. • The superior fibular retinaculum is a short band that extends from the back of the lateral malleolus to the deep transverse fascia of the leg and the lateral surface of the calcaneus. Damage to the retinaculum can lead to instability of the tendons of fibularis longus and brevis. • The inferior fibular retinaculum is continuous in front with the inferior extensor retinaculum, and is attached posteriorly to the lateral surface of the calcaneus. Some of its fibres are fused with the periosteum on the fibular trochlea (peroneal trochlea or tubercle) of the calcaneus, forming a septum between the tendons of fibularis longus and brevis.
- 41. Lateral Ligaments ("T" shaped) • Anterior talofibular (weakest and most frequently injured) • Calcaneofibular (strongest of the three ligaments) • Posterior talofibular Lateral It consist of three bands namely
- 42. Specialised adipose tissue • Heal and metatarsal pads. • The heel is subject to repeated high impacts and is anatomically adapted to withstand these pressures. • The adult heel pad has an average thickness of 18 mm and a mean epidermal thickness of 0.64 mm (dorsal epidermal thickness averages 0.069 mm). • The heel pad contains elastic adipose tissue organized as spiral fibrous septa anchored to each other, to the calcaneus and to the skin. • The septa are U-shaped, fat-filled columns designed to resist compressive loads and are reinforced internally with elastic diagonal and transverse fibres, which separate the fat into compartments.
- 43. • In the forefoot, the subcutaneous tissue consists of fibrous lamellae arranged in a complex whorl containing adipose tissue attached via vertical fibres to the dermis superficially and the plantar aponeurosis deeply. • The fat is particularly thick in the region of the metatarsophalangeal joints, which cushions the foot during the toe-off phase of gait (see below). • Like the heel pad, the metatarsal fat pad is designed to withstand compressive and shearing forces. • Atrophy of either may be a cause of persistent pain in the distal plantar region.
- 44. JOINTS • 33 joints and 26 bones. • Two major joints • The Ankle Joint • The second major joint is the Subtalar Joint T MMLM
- 45. Ankle Joint • The ankle joint is a synovial joint of hinge variety, approximately uniaxial. • The lower end of the tibia and its medial malleolus, together with the lateral malleolus of the fibula and inferior transverse tibiofibular ligament, form a deep recess (‘mortise’) for the body of the talus. • Structurally it is a strong joint and stability is ensured by close interlocking of articular surface, strong collateral ligament and tendon that cross the joint.
- 47. Ankle Joint • Ligaments – Fibrous Capsule – The Deltoid or medial Ligament – A lateral ligament • Fibrous Capsule – Surrounds the joint – Weak anteriorly and posteriorly to allow hinge movement – Attached all around the articular margins except • Posterosuperiorly attached to inferior tibiofibular ligament • Anteroinferiorly attached to dorsum of the neck of the talus at some distance from trochlear surface
- 48. • Deltoid Or Medial Ligament – It is a strong, triangular band, attached to the apex and the anterior and posterior borders of the medial malleolus. It consist of superficial and deep part. – Excessive tensile force results in avulsion fracture rather than a tear of ligament
- 49. The Deltoid Ligament • Deltoid ligament is a combination of: – Anterior talotibial – Tibionavicular – Tibiocalcaneal – Posterior talotibial Medial
- 52. SubTalar Joint • 3 joints between talus and calcaneum namely posterior, anterior and medial. • The posterior joint is named talocalcanean or subtalar joint. • Anterior joints is part of talocalcaneonavicular joint. • Since the three joints form a single functional unit, clinicians often include these joints under the term subtalar joint.
- 53. • However, the sinus tarsi seperates posterior articulation from the anterior and medial articulations. • The greater part of the talocalcaneonavicular joint lies in front of the head of the talus and not below it.
- 55. Talocalcanean Joint • It is a plain synovial joint between the concave facet on inferior surface of the body of talus and convex facet on superior surface of the calcaneum. • The Bones are connected by:- – A fibrous capsule – The lateral and medial talocalcanean ligaments – The interosseous talocalcanean ligament – The cervical ligament
- 56. Interosseous talocalcanean ligament • it is thick and very strong. • It is the chief bond of union between talus and calcaneum. • Occupies sinus tarsi • Seperates talocalcanean joint from talocalcaneonavicular joint. • Becomes taut in eversion and limits this movement
- 58. • Cervical ligament:- – It is placed lateral to sinus tarsi. – It becomes taut in inversion and limits this movement. • Collateral ligaments of ankle joint provide stability to the talocalcanean joint. • Movement – Inversion and Eversion
- 60. Talocalcaneonavicular Joint • Some features of ball and socket joint • Head of talus fits into a socket formed partly by navicular bone and partly by calcaneum. • Two ligaments also take part in forming the socket – Medially by the spring ligament – Laterally by medial limb of bifurcate ligament
- 61. • Bones are connected by fibrous capsule • Movements – Inversion – Eversion
- 62. Spring Ligament • A/k/a Plantar calcaneonavicular ligament • It is powerful • Attached posteriorly to anterior margin of substentaculum tali, and anteriorly to the plantar surface of the navicular bone. • Head of talus rest directly on the upper surface of the ligament. • Plantar surface supported by tendon of tibialis posterior medially and by tendons of flexor hallucis longus and flexor digitorum longus, laterally. • Most Important ligament for maintaining medial longitudinal arch of foot.
- 64. Calcaneocuboid Joint • Saddle Joint. • Articular surface of calcaneum and cuboid is concavoconvex. • Bones are connected by – A fibrous capsule – The lateral limb of the bifurcate ligament – The long plantar ligament – The short plantar ligament
- 66. • Bifurcate Ligament – Y shaped – Stem attached to anterolateral part of sulcus calcanei – Medial limb/ calcaneonavicular ligament attached to dorsolateral surface of navicular bone – Lateral limb/ calcaneocuboid ligament attached to dorsomedial surface of cuboid bone
- 68. • Long Plantar Ligament is a long and strong ligament whose importance in maintaining arches of foot. • It is attached to plantar surface of calcaneum posteriorly and cuboid bone anteriorly. • Short plantar ligament lies deep to the long plantar ligament. • It is broad and strong ligament extending from anterior tubercle of calcaneus to plantar surface of cuboid bone.
- 70. Inversion And Eversion Of Foot • Inversion is movement in which the medial border of the foot is elevated, so that sole faces medially. • Eversion is a movement in which the lateral border of foot is elevated, so that the sole faces laterally. • The movement can be performed voluntarily only when foot is off the ground. When foot is on the ground these movement help to adjust foot to uneven ground.
- 71. • In these movements the entire part of the foot below the talus moves together. • It mainly takes place at the subtalar and talocalcaneonavicular joints and partly at the transverse tarsal joint. • Inversion is accompanied by plantarflexion of the foot and adduction of forefoot. • Eversion is accompanied by dorsiflexion of the foot and abduction of the forefoot.
- 73. • Joints Taking Part – Main • Subtalar (talocalcanean) • Talocalcaneonavicular – Accessory • Transvese tarsal which includes calcaneocuboid and talonavicular joints • Muscle Producing movement – Inversion: Tibialis Anterior and Tibialis Posterior – Eversion: Peroneus Longus and Peroneus Brevis
- 74. • Limiting Factors – Inversion • Tension of peronei • Tension of cervical ligament – Eversion • Tension of tibialis anterior • Tension of tibialis posterior • Tension of deltoid ligament
- 75. • Inversion and eversion greatly help the foot in adjusting to uneven and slippery ground. When feet are supporting weight, these movement occur in a modified form called supination and pronation, which are forced on the foot by the body weight
- 76. Smaller Joints of forefoot • These are plane joints between the navicular, the cuneiforms, the cuboid and the metatarsal bones. • They permit small gliding movements, which allow elevation and depression of the heads of the metatarsals as well as pronation and supination of the foot. • There are 6 joint cavities of the foot (talocalcanean, talocalcaneonavicular, calcaneocuboid, 1st cuneometatarsal, cubometatarsal and calcaneonavicular with extension i.e. navicular with three cuneiforms and 2nd and 3rd cuneometatarsal)
- 78. TarsoMetatarsal Joint • Tarsometatarsal articulations are approximately plane synovial joints. • The joints are approximately on an imaginary line traced from the tubercle of the fifth metatarsal to the tarsometatarsal joint of the great toe, except for that between the second metatarsal and intermediate cuneiform, which is 2–3 mm proximal to this line. • Movements between the tarsals and metatarsals are limited to flexion and extension, except in the first tarsometatarsal joint, where some abduction and rotation occur.
- 79. Metatarsophalangeal Joint • Metatarsophalangeal articulations are ovoid or ellipsoid joints between the rounded metatarsal heads and shallow cavities on the proximal phalangeal bases. They are usually 2.5 cm proximal to the web spaces of the toes. • Flexion, extension, abduction and adduction are the movements that occur in this joints
- 80. Interphalangeal Joint • Interphalangeal articulations are almost pure hinge joints, in which the trochlear surfaces on the phalangeal heads articulate with reciprocally curved surfaces on adjacent phalangeal bases. • Flexion and extension occurs in this joints
- 81. Muscles • Extension of deep fascia form intermuscular septa that divide leg into compartments. • The anterior and posterior intermuscular septa are attached to anterior and posterior borders of fibula dividing leg into anterior, posterior and lateral compartment. • The posterior compartment is further subdivided into superficialand deep parts by transverse intermusclar septum
- 82. Muscle Compartments • Anterior Compartment (Dorsal flexors) – Tibialis anterior – Peroneous tertius – Extensor digitorum Longus – Extensor digitorum brevis – Extensor hallicus longus • Lateral Compartment (Evertors) – Peroneus longus – Peroneus brevis
- 83. Muscle Compartments • Deep Posterior Compartment (Plantar Flexors) – Flexor digitorum longus – Flexor hallicus – Tibialis Posterior • Superficial Posterior Compartment(Plantar Flexors) – Gastrocnemius – Soleus – Plantaris
- 84. Ankle and Foot Muscles • Superficial Posterior Compartment – Gastrocnemius – Soleus – Plantaris • Deep Posterior Compartment – Flexor digitorum longus – Flexor hallicus – Tibialis Posterior • Lateral Compartment (Evertors) – Peroneus longus – Peroneus brevis • Anterior Compartment (Dorsal flexors) – Tibialis anterior – Peroneous tertius – Ext. dig. Longus – Ext. hallicus
- 85. Gastrocnemius • Origin: posterior surface of the two femur condyels • Insertion: posterior surface of the calcaneus via Achilles tendon • Actions: – plantar flexion of the foot – flexion of the knee • Stronger plantar flexion when the knee is extended • Superficial posterior compartment Posterior
- 86. Soleus • Located beneath the gastrocnemius • Origin: upper 2/3 of the posterior surfaces of the tibia and fibula • Insertion: posterior surface of the calcaneus via Achilles tendon • Action: – plantar flexion • Superficial posterior compartment Posterior
- 87. Gastrocnemius & Soleus •Gastronemius and Soleus = “triceps surae” due to their three heads
- 89. Achilles Tendon • Named after Achilles • Largest tendon • 1000 pounds of force • Tendon of the Gastrocnemius and Soleus
- 90. Plantaris • Absent in some humans • Origin: lateral epicondyle • Insertion: calcaneus • Actions: – plantar flexion • Superficial posterior compartment Posterior
- 92. Tibialis posterior • Origin: posterior surface of the upper half of the adjacent surface of tibia & fibula • Insertion: navicular, cuneiforms, and cuboid bones and bases of the 2nd-5th metatarsal bones. • Note: passes posterior to medial malleolus. • Actions: – plantar flexion – inversion of the foot • Deep posterior compartment Posterior
- 93. Flexor Digitorum Longus • Origin: middle 1/3 of the posterior surface of the tibia • Insertion: base of the distal phalanges of each of lateral four toes • Note: passes posterior to medial malleolus. • Actions: – toe flexion – plantar flexion, – inversion of the foot • Maintains the longitudinal arch • Deep posterior compartment Posterior
- 94. Flexor Hallicus Longus • Origin: middle half of the posterior surface of the fibula • Insertion: distal phalanx of the large toe, plantar surface • Note: passes posterior to medial malleolus. • Actions: – Flexion of the great toe – Inversion – Plantar flexion • Deep posterior compartment Posterior
- 96. Tibialis anterior • Origin: upper 2/3 of the anterior surface of the tibia • Insertion: medial cuneform and the first metatarsal • Note: passes anterior to medial malleolus. • Actions: – Dorsal flexion – Inversion. • Anterior compartment Anterior
- 97. Extensor hallicus longus • Origin: middle 2/3 of the inner surface of the front of the fibula • Insertion: top of the distal phalanx of the great toe • Note: passes anterior • Actions: – Extension of big toe – Dorsiflexion – Weak inversion of the foot • Anterior compartment Anterior
- 98. Extensor digitorum longus • Origin: lateral condyle of the tibia and anterior surface of the fibula • Insertion: middle and distal phalanges of the four lateral toes. • Note: passes anterior to lateral malleolus. • Actions: – Toe extension – Dorsiflexion – Eversion • Anterior compartment Anterior
- 99. Extensor Digitorum Brevis • Origin: Anterior part of the superior surface of the calcaneum • Inserion: middle and distal phalanges of the four medial toes. • Note: Medial most part of muscle which is distict is known as extensor hallucis brevis • Action: – Toe Extension • Anterior Compartment
- 100. Peroneous tertius • Origin: lower fibula • Insertion: dorsal surface of the 5th metatarsal • Note: passes anterior to lateral malleolus. • Action: – Dorsiflexion – Eversion • Anterior compartment Anterior
- 102. Peroneus longus muscle • Origin: head and upper 2/3 of the outer surface of the fibula • Insertion: undersurfaces of the 1st cuneiform and first metatarsal bones • Note: passes posterior to lateral malleolus. • Actions: – Eversion – Plantar flexion • The tendon goes under the foot from the lateral to the medial surface, thus aiding in support for the transverse arch. • Lateral compartment Lateral
- 103. Peroneus brevis muscle • Origin: lower 2/3 of the outer surface of the fibula • Insertion: dorsal surface of the 5th metatarsal • Note: passes posterior to lateral malleolus. • Actions: – Plantar flexion – Eversion • Anterior compartment Lateral
- 104. Lateral Compartment
- 105. Muscles and Tendons of the Sole • Four Layers • Muscles of the 1st layer – Flexor digitorum brevis – Abductor hallucis – Abductor digiti minimi • Muscles of the 2nd Layer – Tendon of the flexor digitorum longus – Flexor hallucis longus – Flexor digitorum accessorius – Lumbrical muscles
- 106. • Muscles of the 3rd layer – Flexor haluucis brevis – Flexor digiti minimi brevis – Adductor hallucis • Muscles of the 4th layer – Interosseous muscles – Tendon of tibialis posterior – Tendon of peroneus longus
- 116. Arches of the Foot • Arches of the foot help in walking, running and jumping. In addition they help in weight bearing and in providing upright posture. • Arches are supported by intrinsic and extrinsic muscles in the sole, ligaments, aponeurosis and shape of the bones. • The Foot has to act :- – As a pliable platform to support weight in the upright posture – As a lever to propel the body forward
- 117. • Classification of Arches – Longitudinal • Medial • Lateral – Transverse • Anterior • Posterior
- 119. Medial Longitudinal Arch • This arch is considerably higher, more mobile and resilient than the lateral. • It is considered as big arch of a small circle. • Acts as a shock absorber. • Anterior end:- Formed by head of 1st, 2nd, 3rd metatarsals. • Posterior End:- Medial tubercle of the calcaneum. • Summit:- Superior articular surface of the body of talus
- 120. • Pillars – Anterior pillar is long and weak, formed by talus, navicular, three cuneiform bones and first three metatarsal bones. – Posterior pillar is short and strong, formed by medial part of the calcaneum • Main Joint:- Talocalcaneonavicular joint • Phalanges do not take part in formation of the arches
- 122. Lateral Longitudinal Arch • Characteristically low and limited mobility. • Built to transmit weight and thrust to the ground. • Considered as small arc of big circle • Ends:- – Anterior:- Heads of 4th and 5th metatarsal bones – Posterior:- Lateral tubercle of the calcaneum • Summit:- articular facets of the superior surface of the calcaneum at the level of sub talar joint
- 123. • Pillars:- – Anterior pillar:- long and weak, formed by cuboid bone and by 4th and 5th metatarsal bones. – Posterior pillar:- short and strong, formed by lateral half of the calcaneum. – Main Joint:- Calcaneocuboid Joint
- 125. Anterior Transverse Arch • Formed by the heads of the five metatarsal bones. • Complete arch, as heads of 1st and 5th come in contact with the ground and forms the two end of the arch
- 126. Posterior Transverse Arch • Formed by the greater part of tarsus and metatarsus. • Incomplete, as only the lateral end comes in contact with the ground forming half dome, which is completed by similar half dome of the opposite foot.
- 127. Factors Responsible for Maintenance of Arches • Shape of the bones concerned • Intersegmental ties/staples or ligaments (and muscles) • The beams or bowstrings that connect two ends of the arch • Slings that keep the summit of the arch pulled up • Suspension
- 128. Bony Factor • Posterior transverse arch is formed and maintained mainly because of the fact that many of the tarsal bones involved (eg. the cuneiform bones) and the heads of the metatarsal bones, are wedge shaped, the apex of wedge pointing downwards. • The bony factor is not very important in the case of other arches
- 129. Intersegmental Ties • All arches are supported by ligaments uniting the bones concerned. • The most important of these are – The spring ligament for the medial longitudinal arch – The long and short plantar ligaments for the lateral longitudinal arch – In the case of transvers arch, the metatarsal bones are held together by the interosseous muscles.
- 130. The Beams • The Longitudinal arches are prevented from flattening by the plantar aponeurosis and by the muscles of the first layer of the sole (Flexor digitorum brevis, flexor digiti minimi and abductor digiti minimi ). • These structure keep the anterior and posterior ends of the arches pulled together.
- 131. Slings • The summit of the medial longitudinal arch is pulled upwards by tendon passing from the posterior compartment of the leg into the sole i.e. tibialis posterior, flexor hallucis longus, flexor digitorum longus. • The summit of lateral longitudinal arch is pulled upwards by peroneus longus and peroneus brevis.
- 132. Slings (cont.) • The tendons of tibialis anterior and peroneus longus together form a sling (stirrup) which keeps the middle of the foot pulled upwards, thus supporting the longitudinal arches. • Peroneus longus runs transversly across the sole, it pulls the medial and lateral margins of the sole closer together, thus maintaining the transverse arch. • The transverse arch is also supported by tibialis posterior which grips many of the bones of the sole through its slips
- 133. Suspension • Medial Longitudinal Arch:- Tibialis Anterior • Lateral Longitudinal Arch:- Peroneus Longus
- 134. Function of Arches • Distribute body weight to the weight to the weight bearing areas of the sole, mainly the heel and the toes. Out of the later, weight is borne mainly on 1st and 5th toe. The lateral border of the foot bears some weight, but this is reduced due to the presence of the lateral longitudinal arch • The arches acts as spring (chiefly the medial longitudinal arch) which are of great help in walking and running
- 135. Function of Arches (cont.) • The act as shock absorbers in stepping and particularly in jumping • The concavity of the arches protects the soft tissues of the sole against pressure • The character of the medial longitudinal arch is resiliency and that of lateral longitudinal arch is rigidity.
- 137. Thank You