Downloaded 17 times

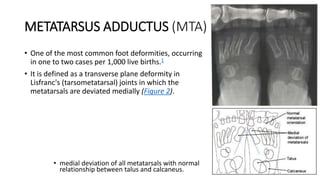
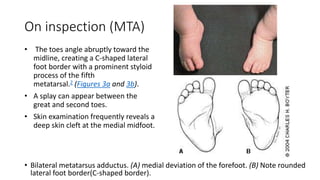
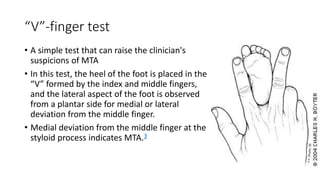
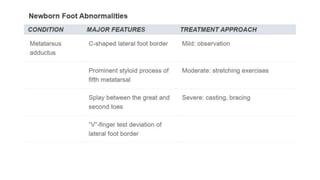
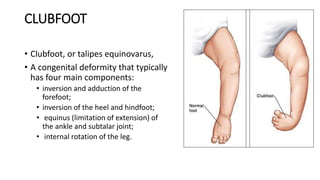
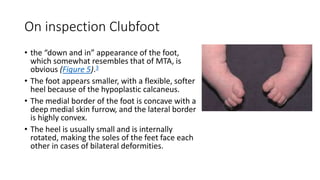

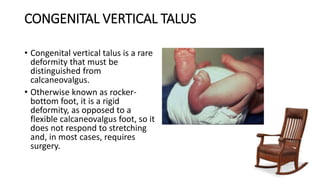
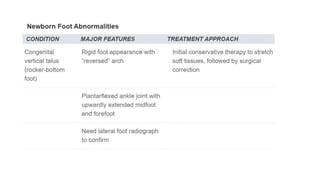
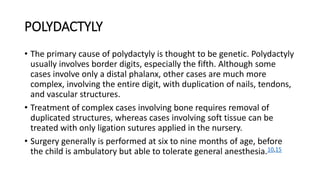

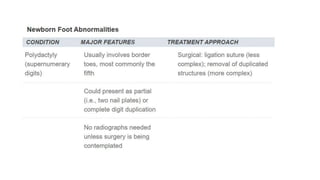

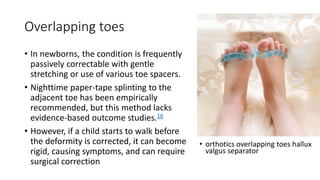
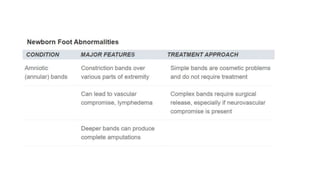

The document provides information about examining and diagnosing common abnormalities in newborn feet. It begins with an overview of the examination process and important structures of the newborn foot. The main part then describes various foot abnormalities like metatarsus adductus, clubfoot, calcaneovalgus, congenital vertical talus, and digital deformities. For each abnormality, it covers appearance, diagnostic tests, and typical treatment approaches, which generally begin with conservative measures like stretching or splinting. Surgery is considered if conservative treatments fail or for more severe cases. The goal of treatment is usually to correct deformities early before they become fixed.



































































