Downloaded 336 times
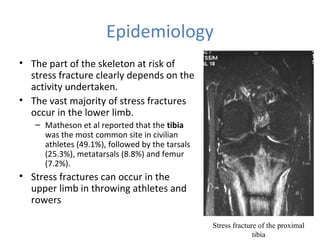
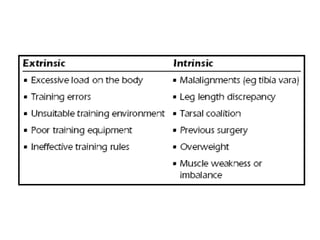





Stress fractures occur when normal bone is exposed to abnormal stress over time. They are common in military personnel and athletes. The document discusses stress fractures, defining them and covering their epidemiology, risk factors, pathophysiology, diagnosis and management. Key points: military service often links to stress fractures due to abrupt increases in training intensity; lower limb bones like the tibia are most commonly affected; overtraining, nutrition deficits and bone anatomy influence risk; MRI is a sensitive diagnostic tool; most stress fractures are managed non-operatively with rest, while displaced fractures may require surgery.


























































![Presentation4[1]](https://cdn.slidesharecdn.com/ss_thumbnails/presentation41-110916142438-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)




























