Download as PDF, PPTX





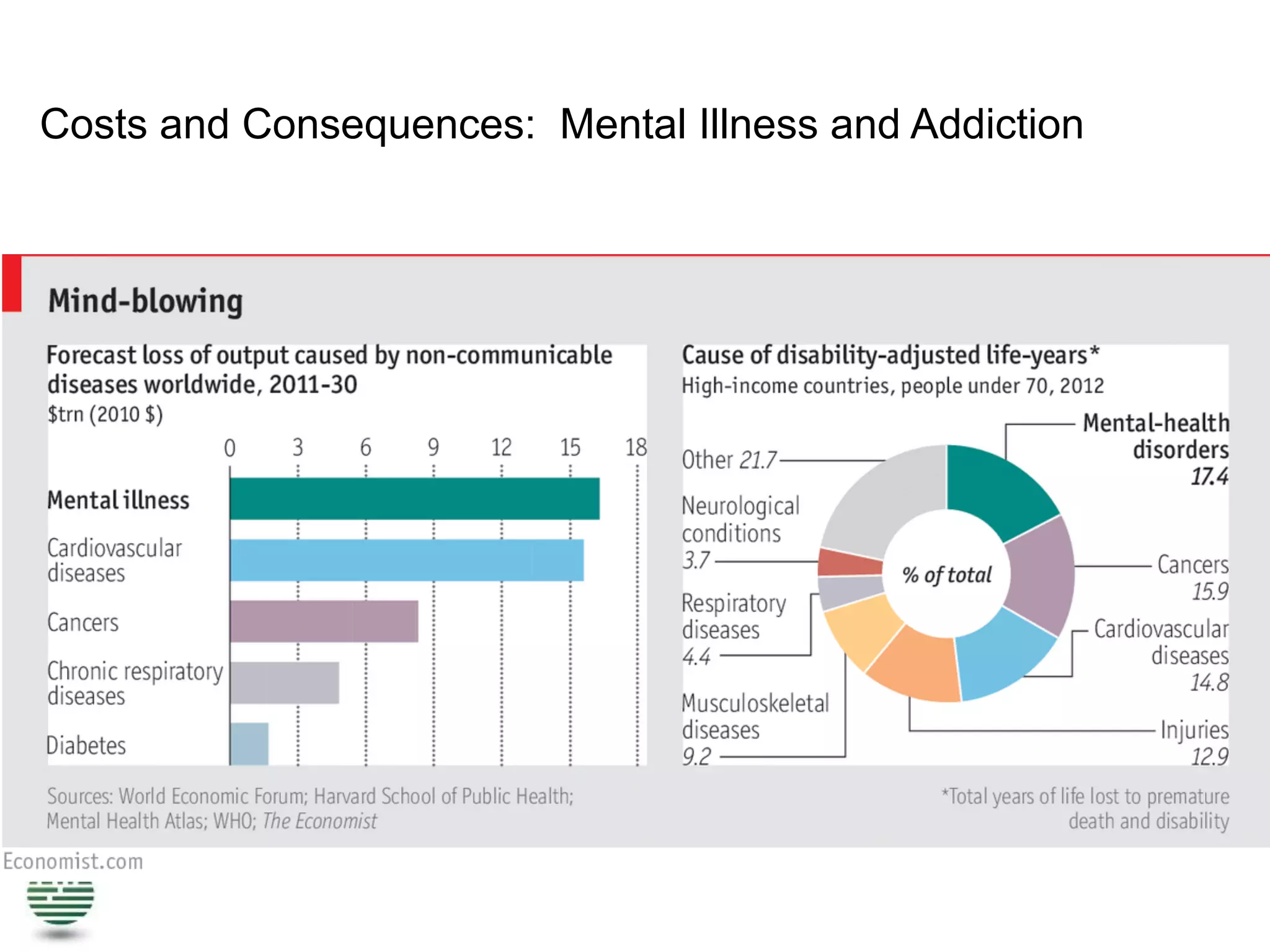
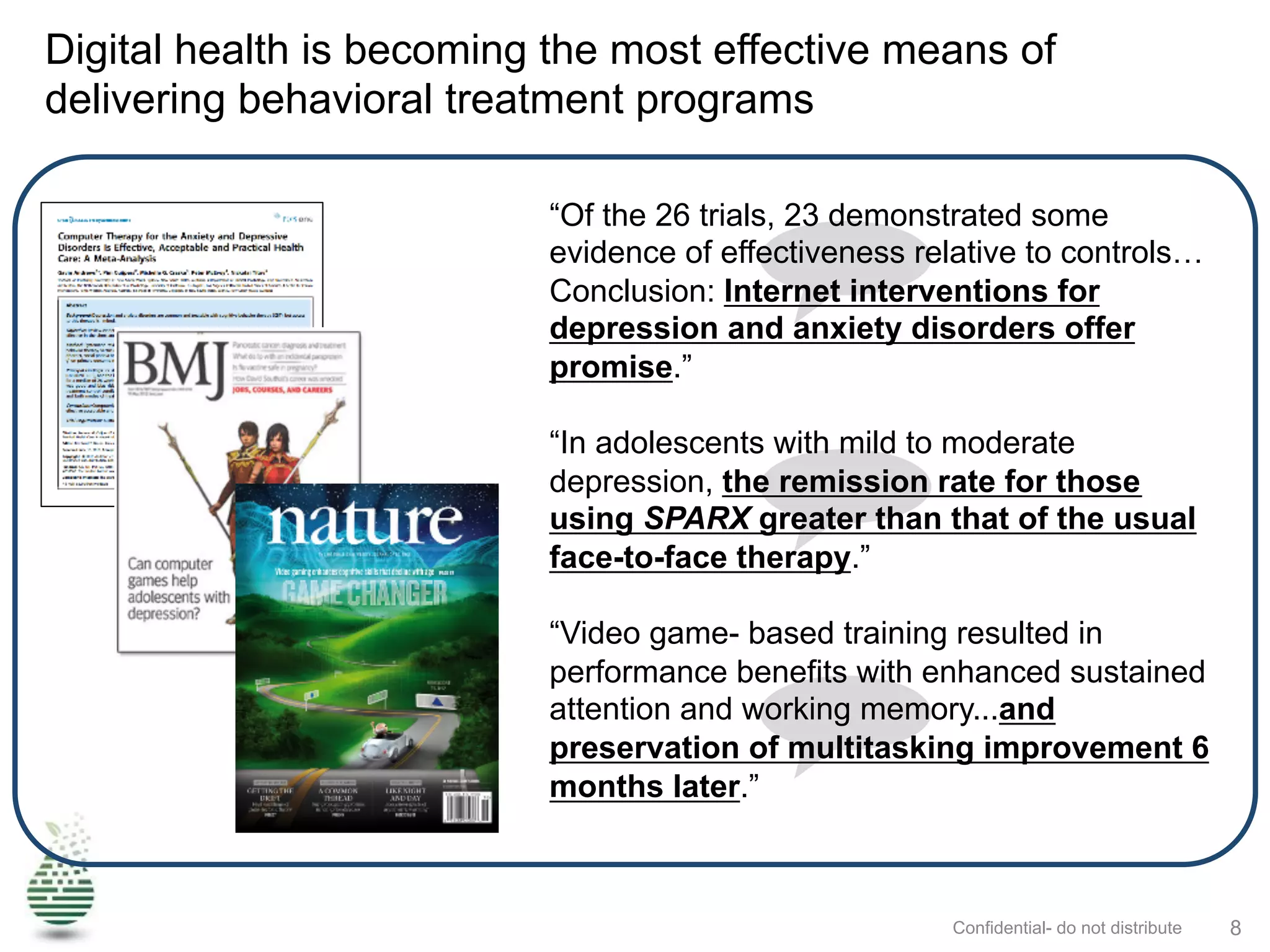
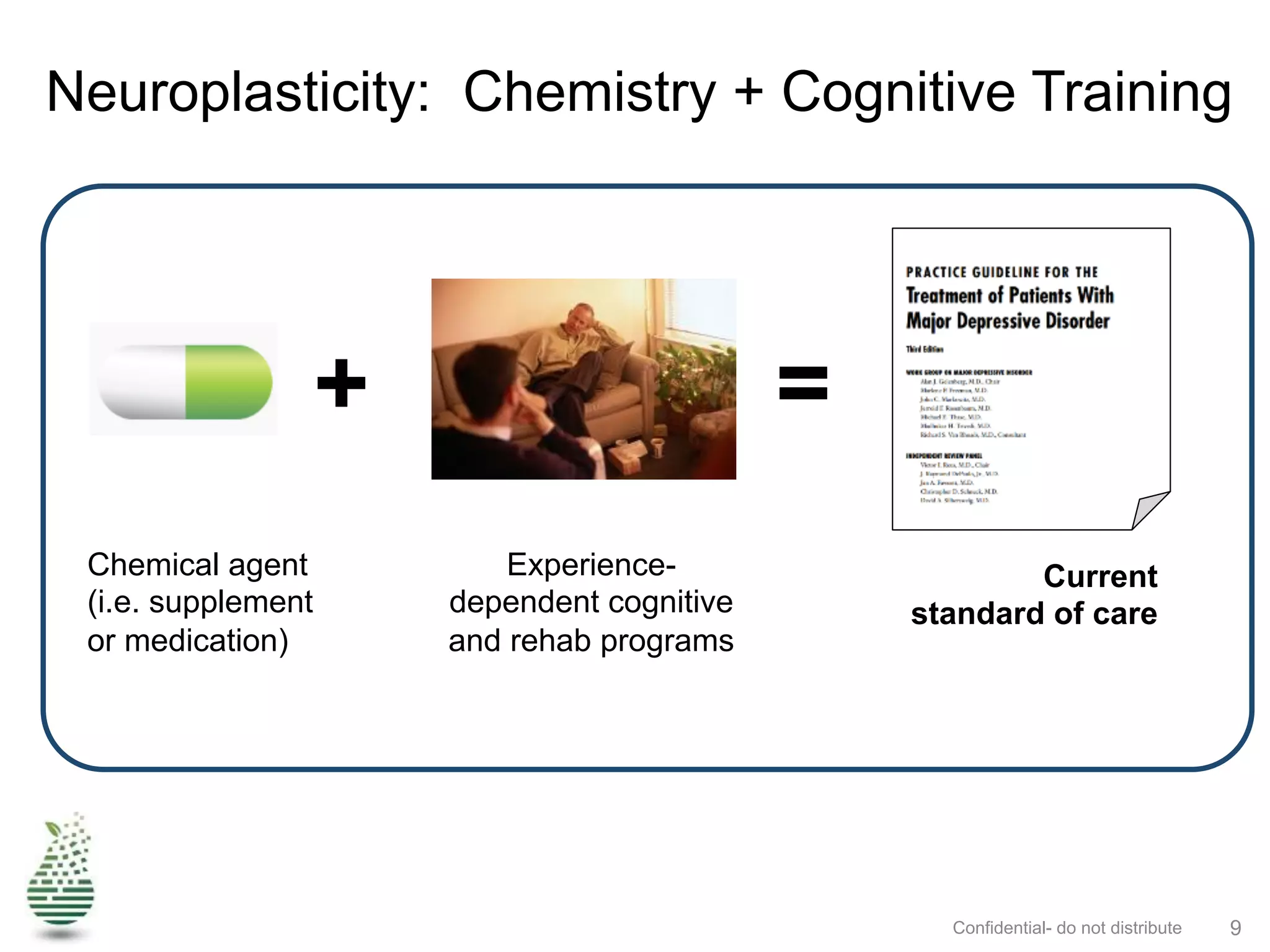
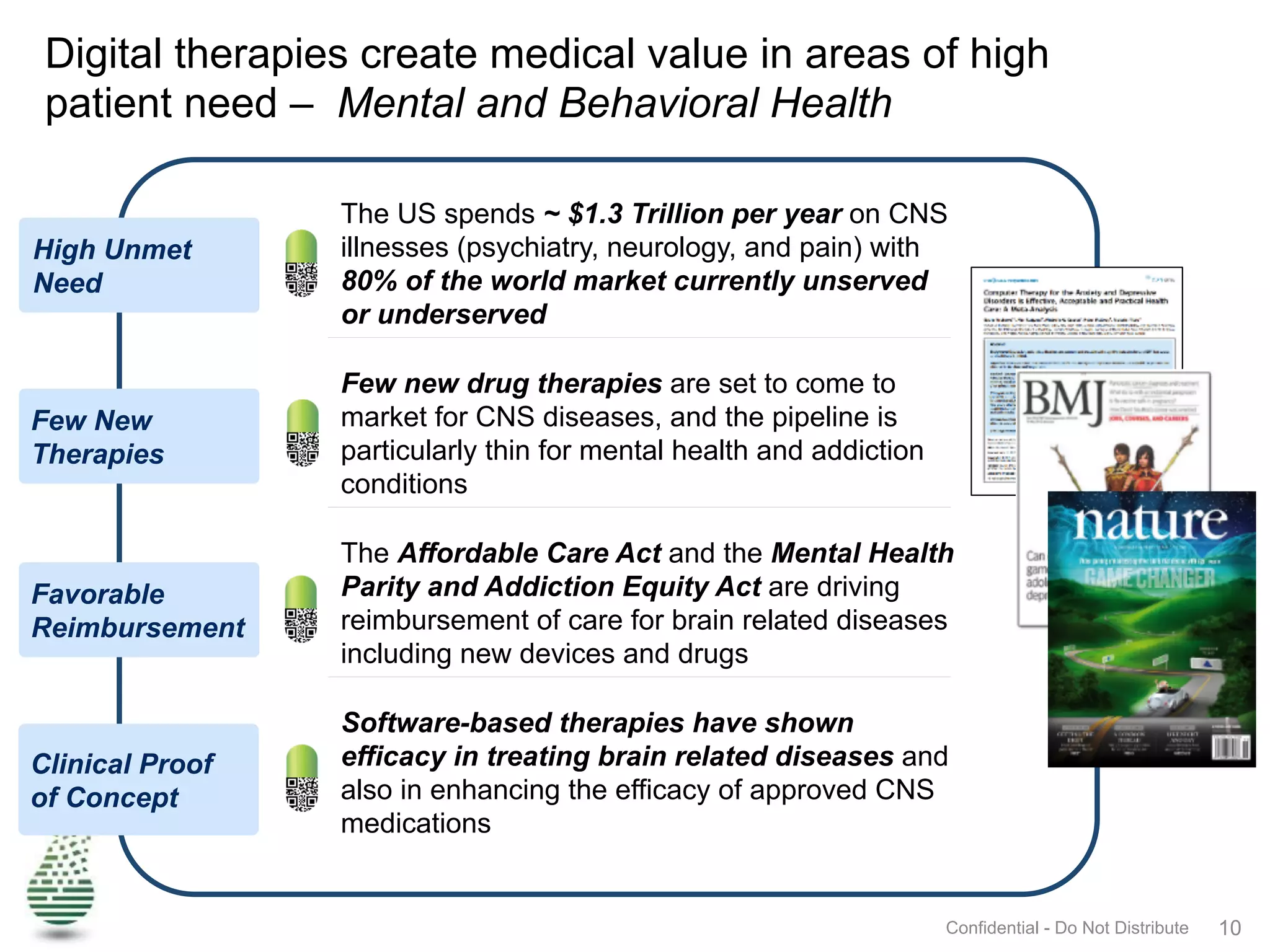





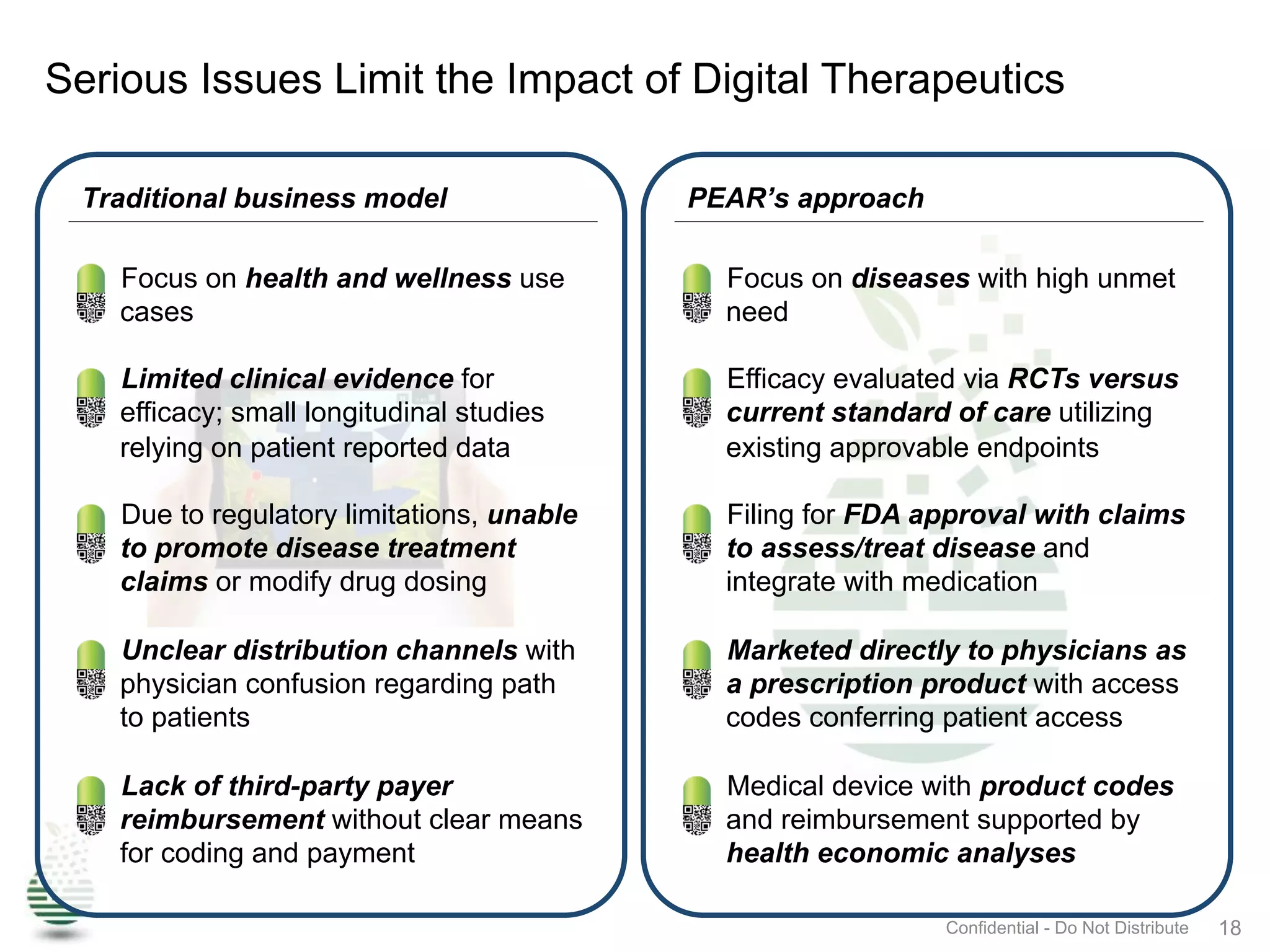




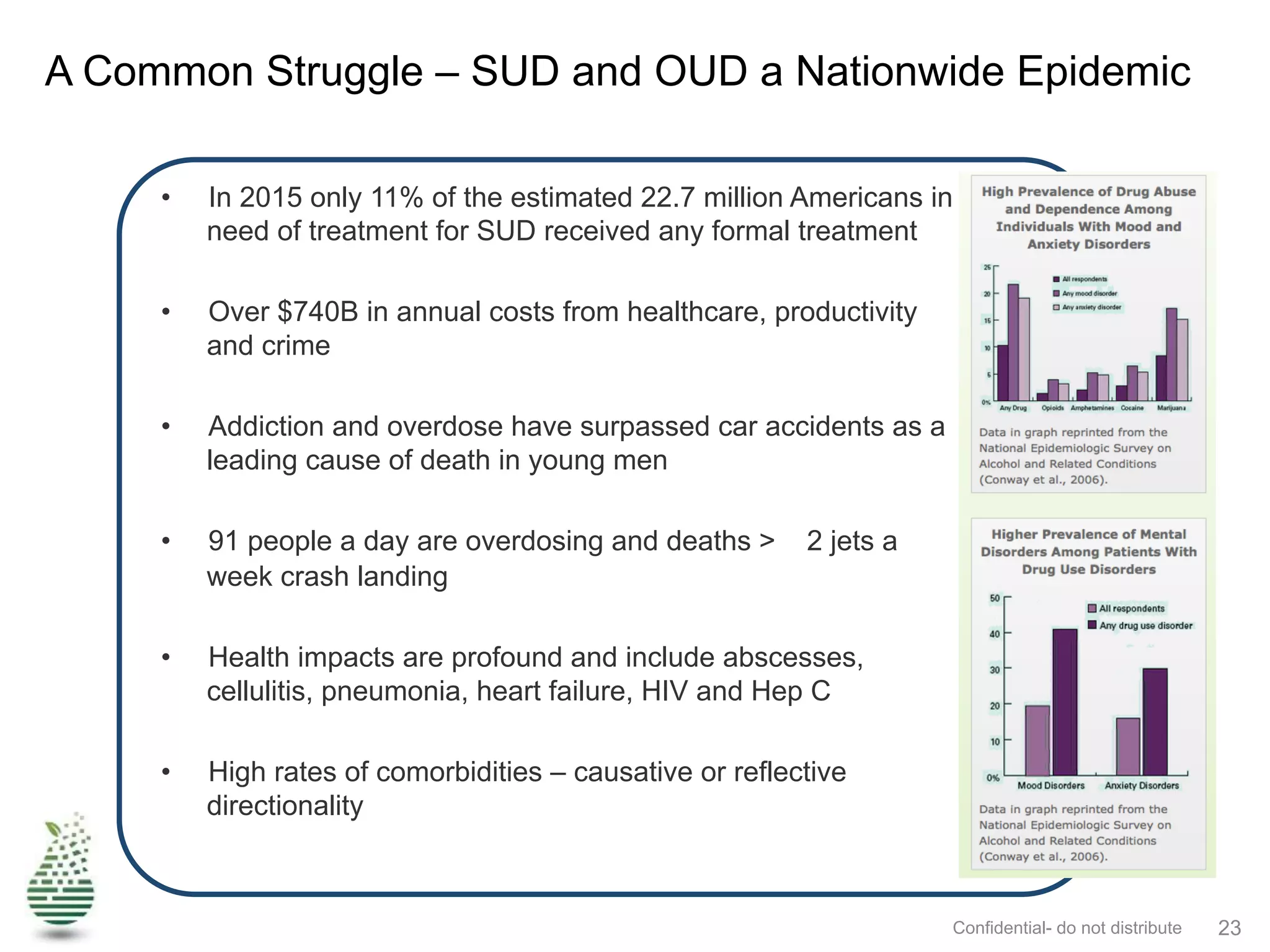



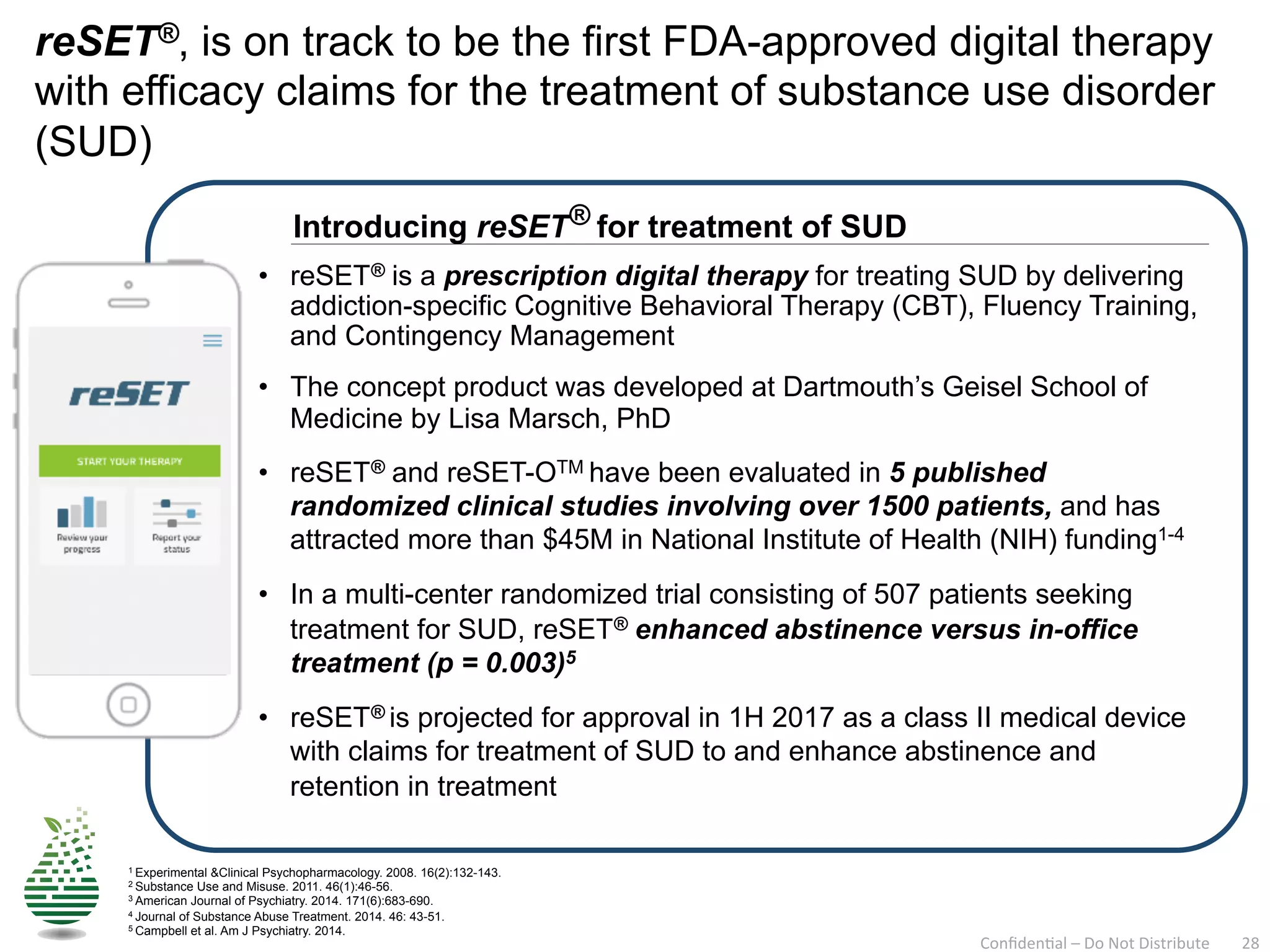














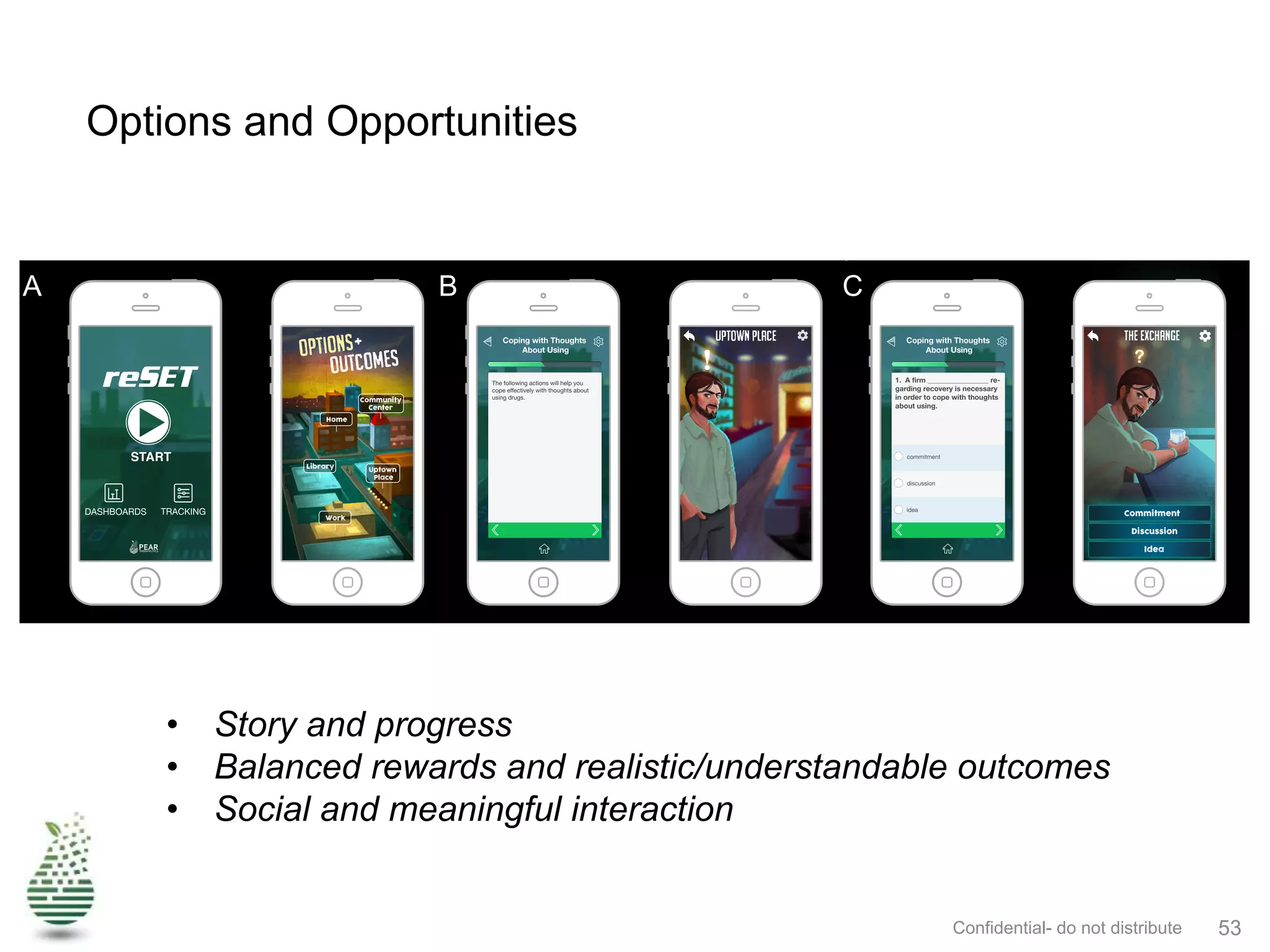



Pear Therapeutics is a leader in developing FDA-regulated digital therapeutics, aiming to treat serious mental health disorders through prescription digital therapies like Reset®, which has shown improvement in abstinence rates for substance use disorder. The company addresses significant unmet needs in brain health treatment, with a focus on providing effective, accessible, and scalable digital health solutions to combat the high economic burden and prevalence of mental illnesses. Additionally, the document outlines the challenges faced in the integration of serious games and apps within regulated healthcare environments, emphasizing the need for clinical evidence and reimbursement models.























































































