Download to read offline

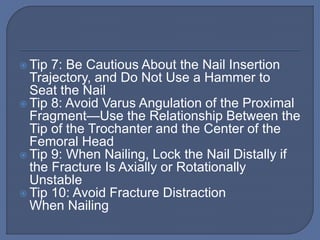

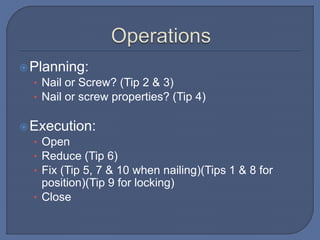
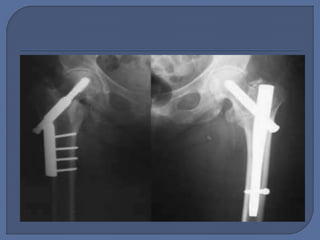
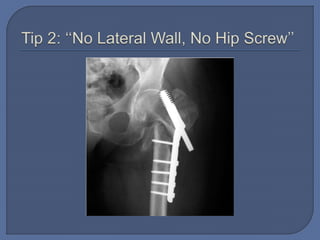
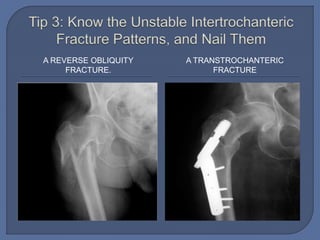
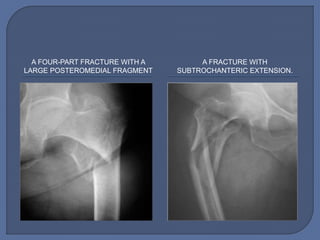
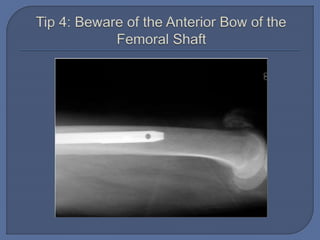
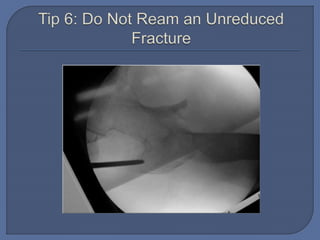
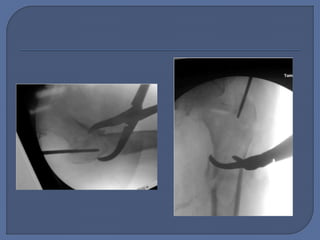
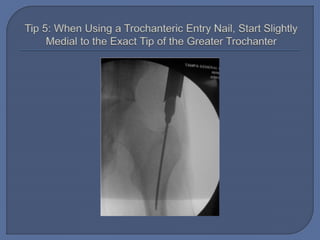
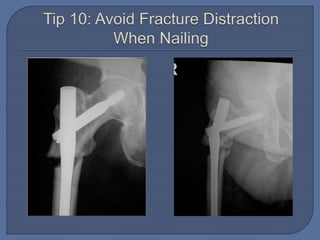
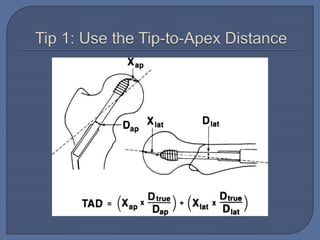
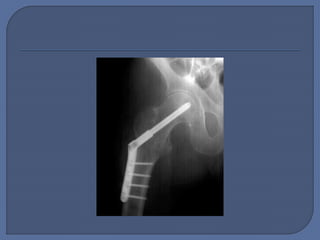
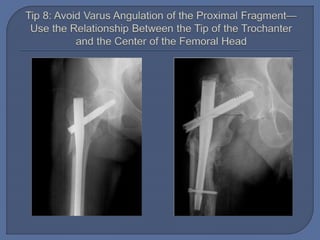




Dr. Abdalla Mutwakil Gamal, a medical officer and orthopedic trauma director with extensive training and over 100 publications, outlines key tips for intertrochanteric fracture management, emphasizing the importance of planning and execution in surgical procedures. Notable instructions include avoiding lateral wall screws, proper placement of nails, and careful attention to fracture stability during treatment. The document serves as a guideline for orthopedic surgeons in optimizing fracture fixation techniques.