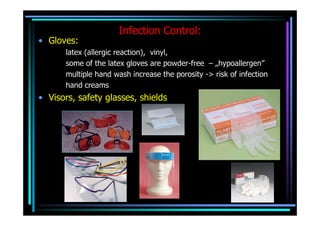
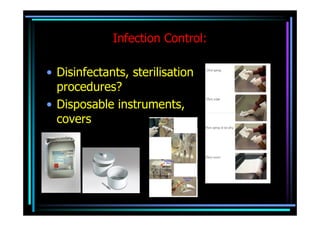
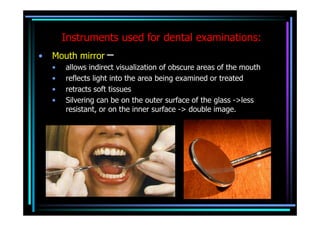
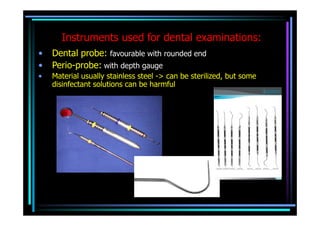
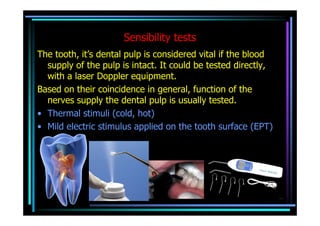
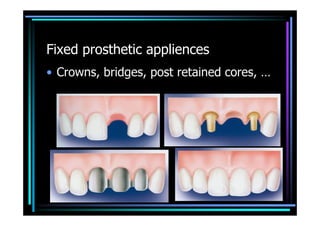
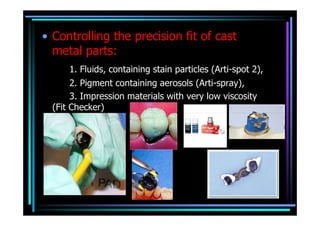
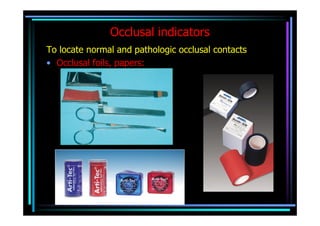
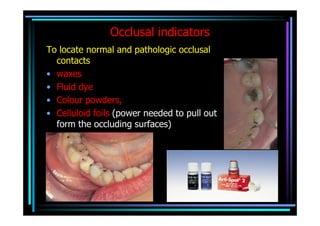
This document discusses various technologies and methods used in dentistry, including infection control protocols using gloves, visors, and sterilization procedures. It also examines instruments used for dental examinations like mirrors, probes, and tools for sensibility tests. Methods for creating bite registrations and indicators for plaque, caries, and occlusion are outlined. Finally, it briefly touches on digital radiology systems and the radioopacity of different dental materials.