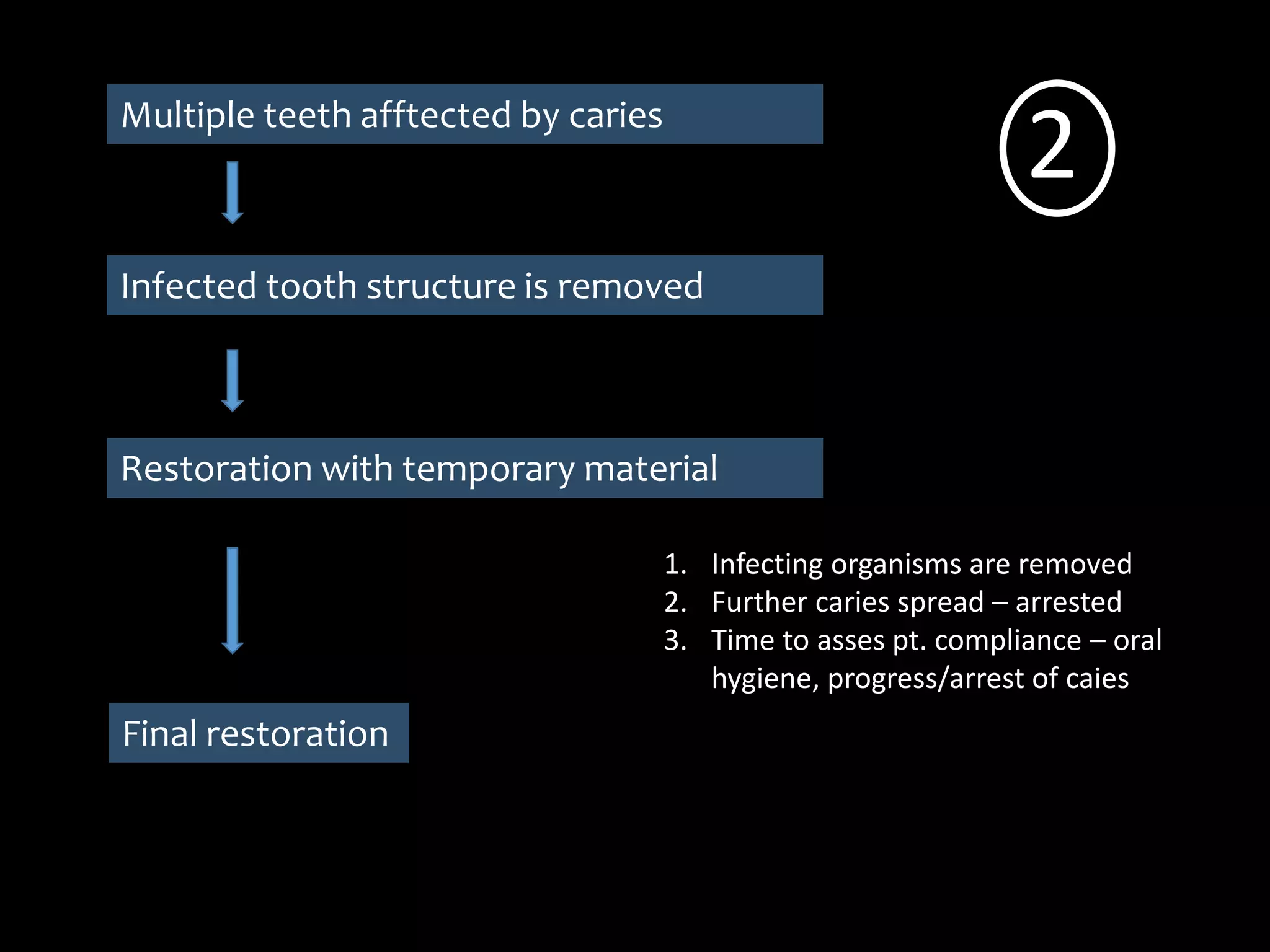
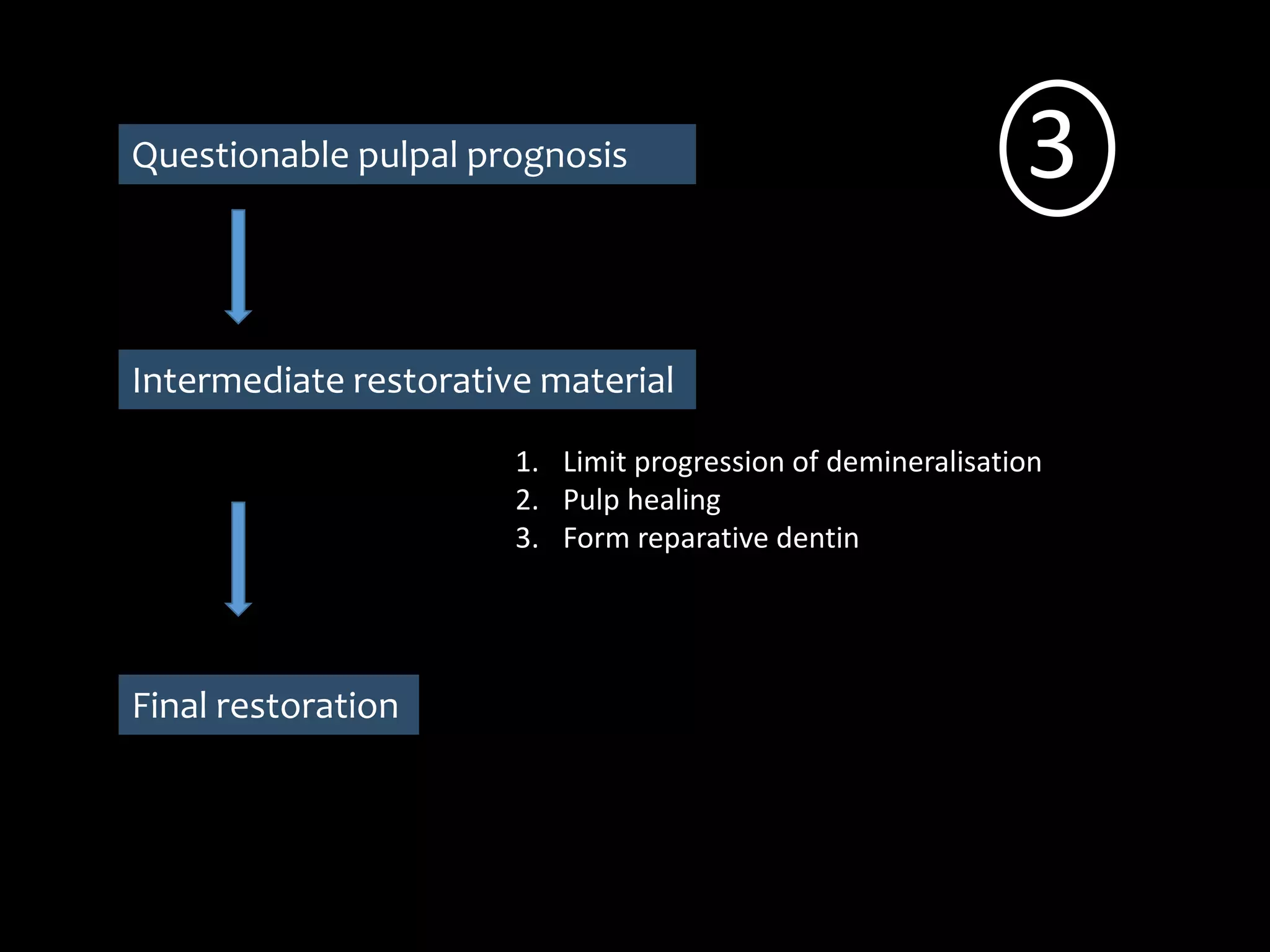
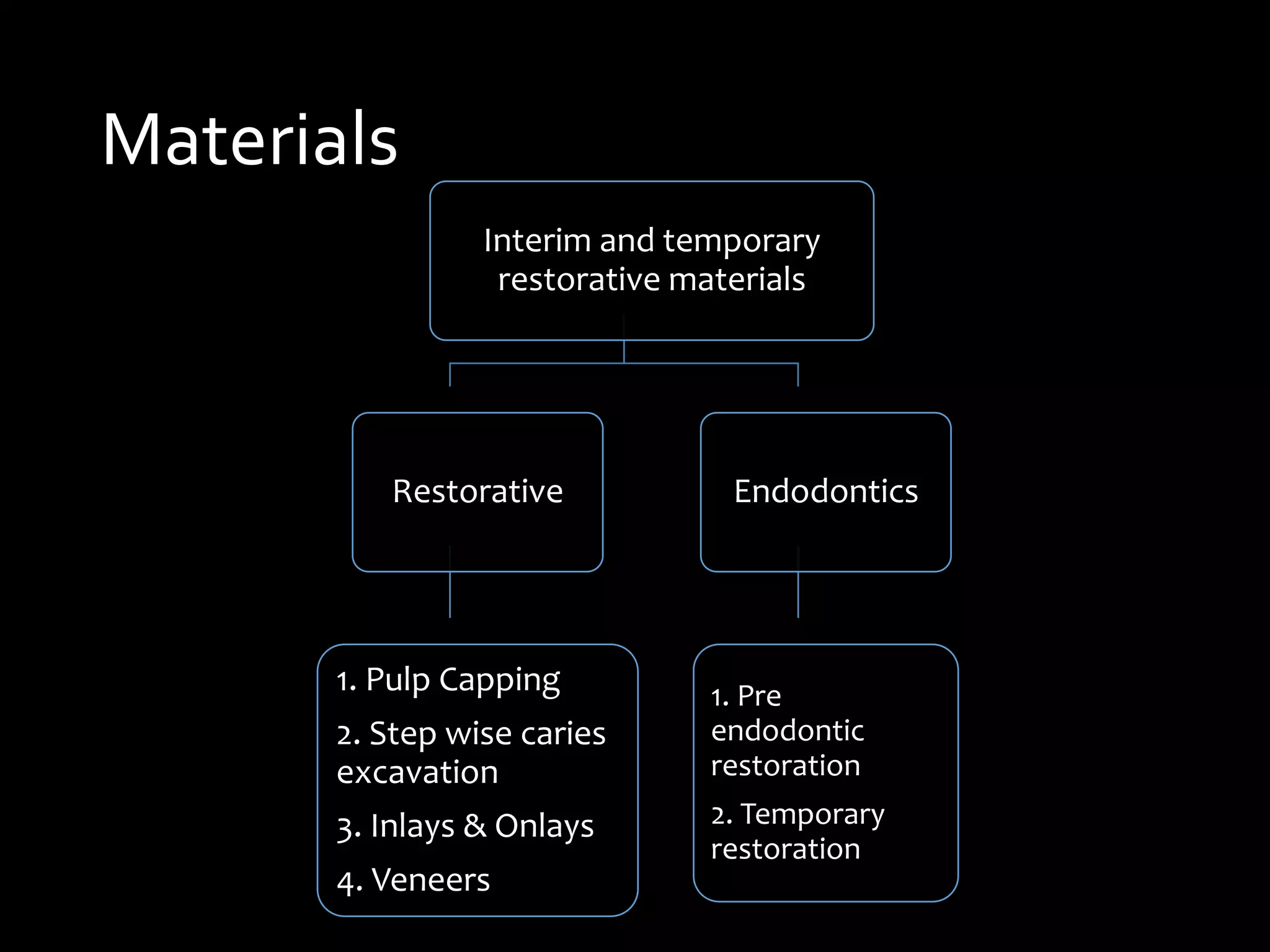
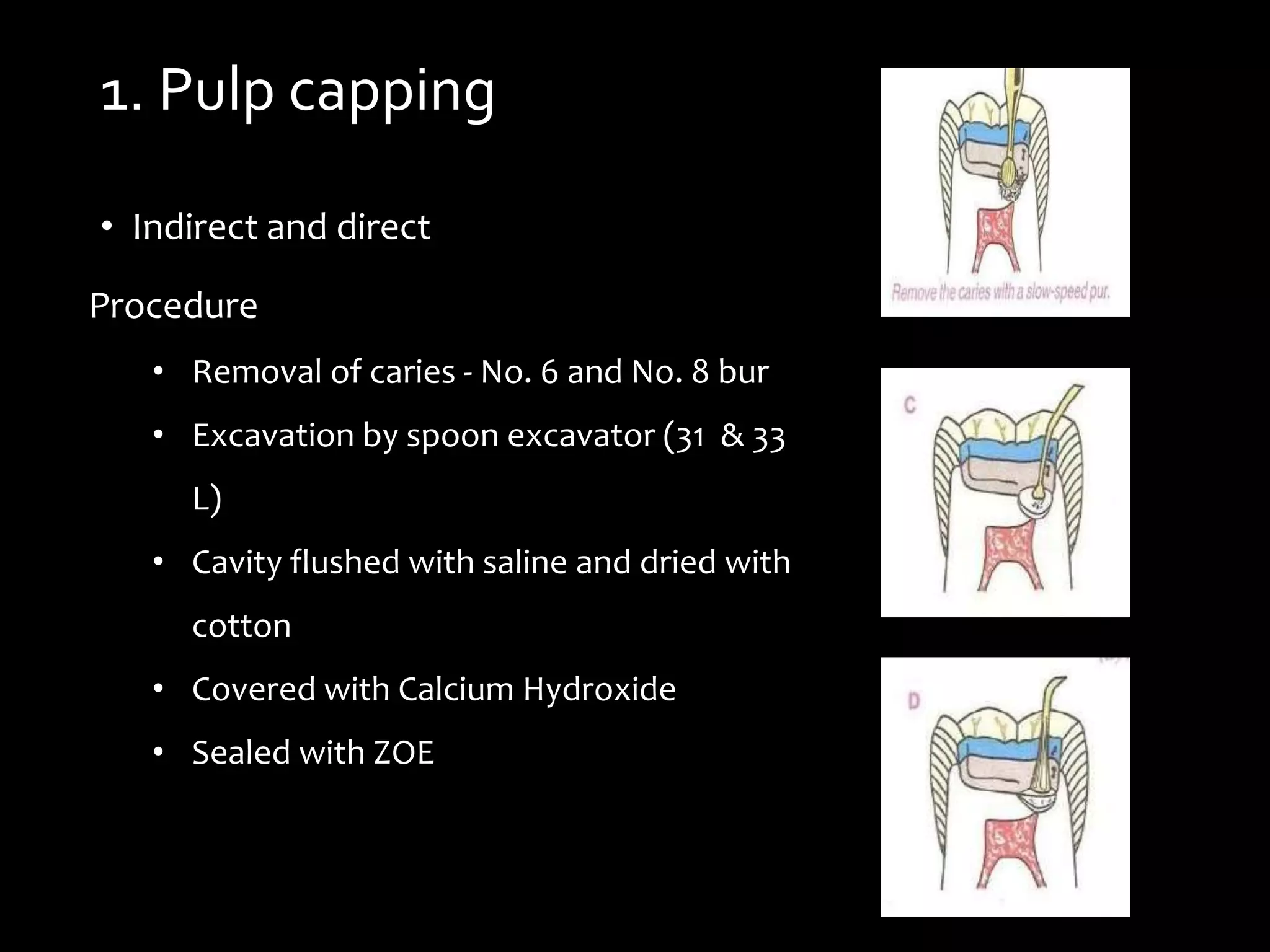
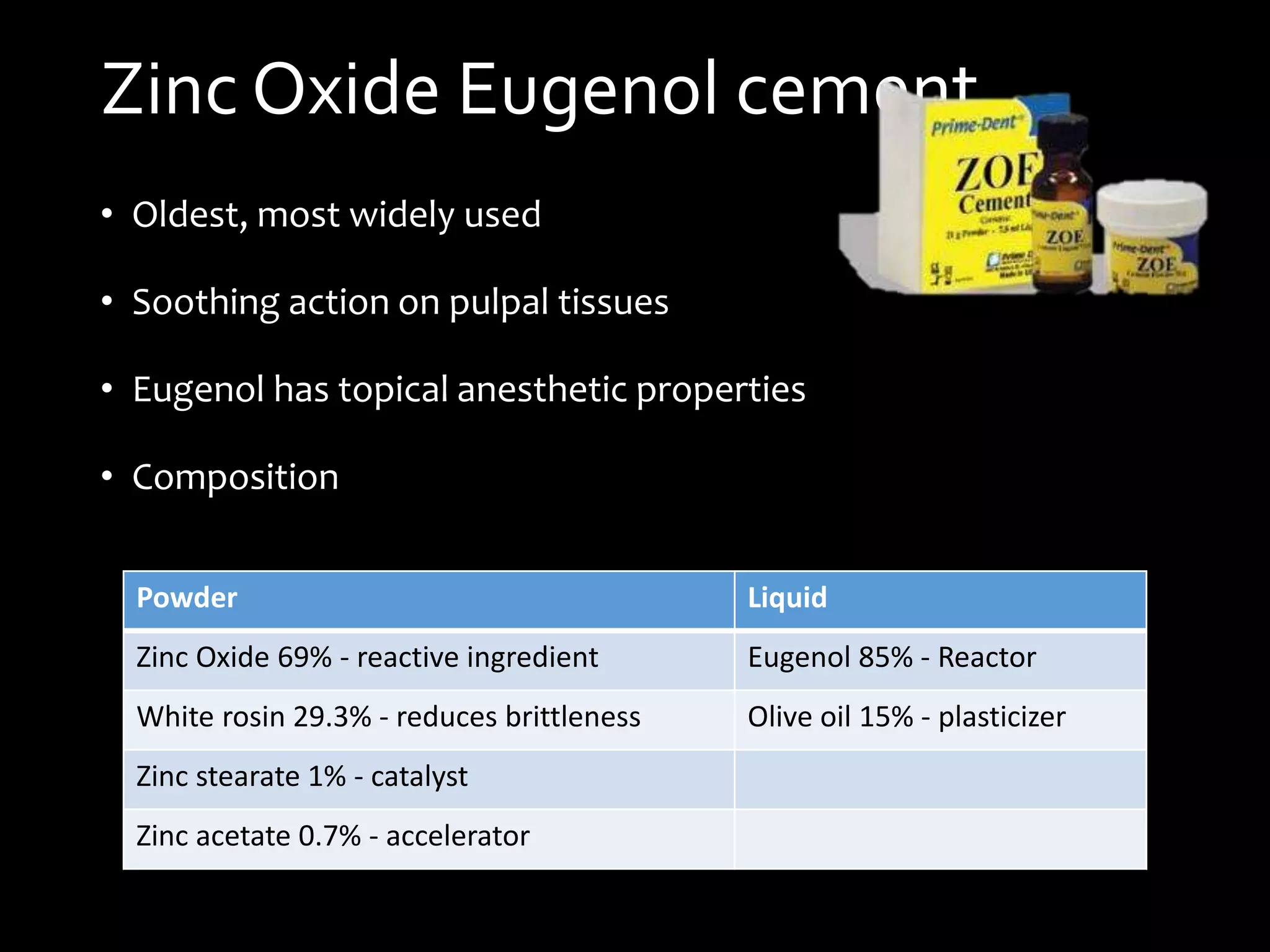
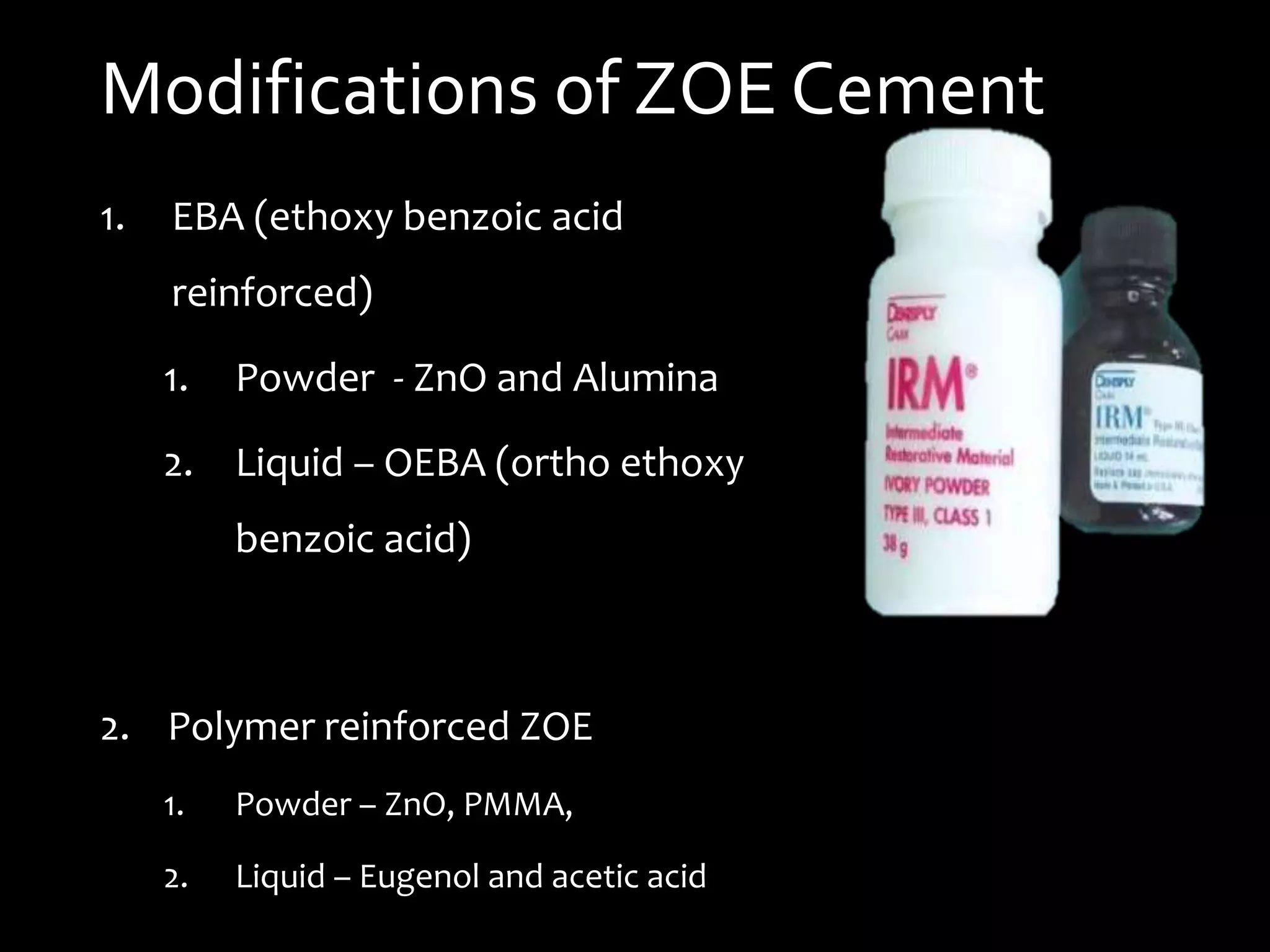
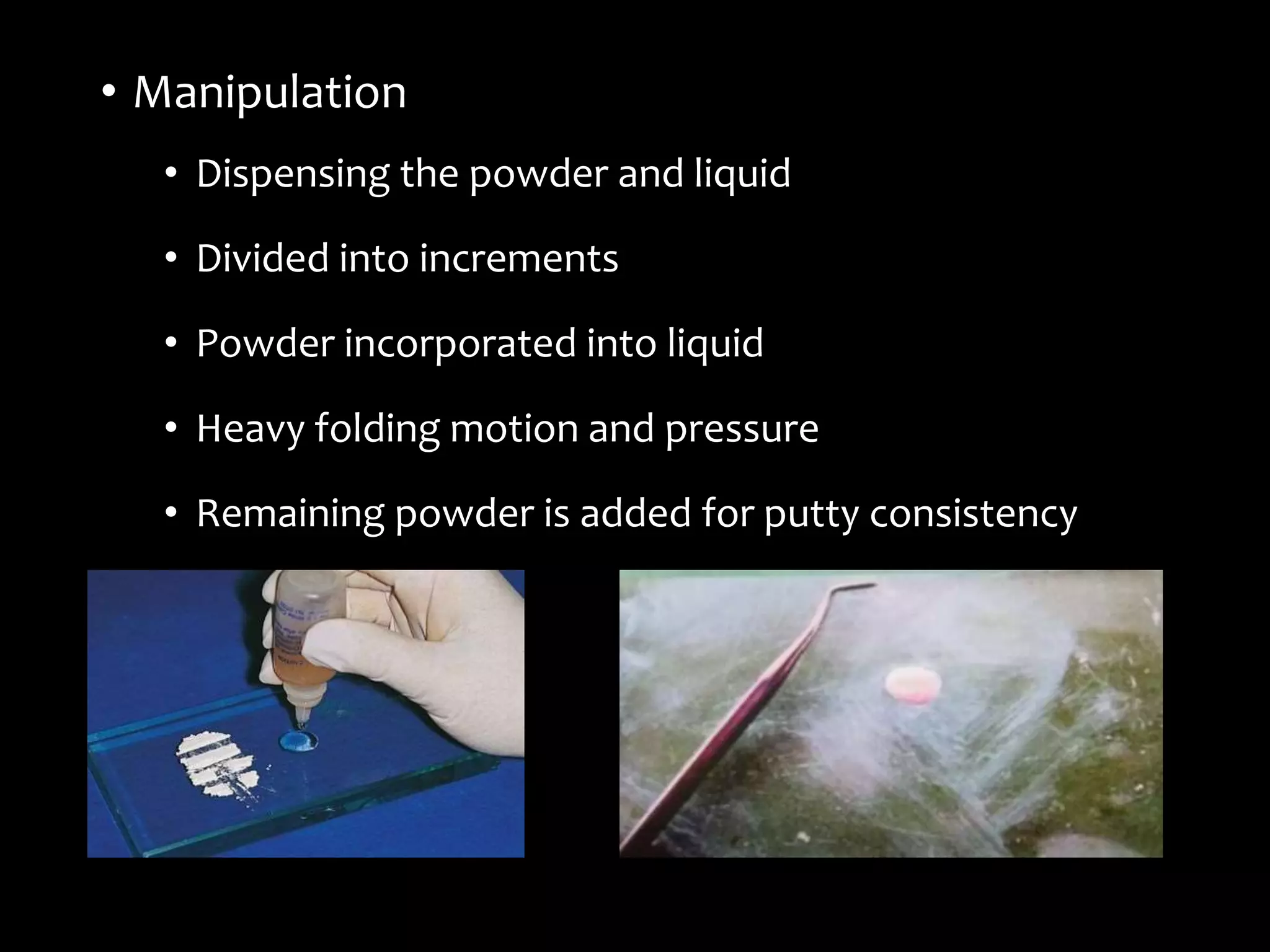
The document provides a comprehensive guide to interim and temporary dental restorations, discussing their objectives, materials, and techniques. Key aspects include maintaining aesthetics, preventing tooth movement, and facilitating treatment evaluation, along with detailing the use of various temporary materials such as zinc oxide eugenol cement and composite resins. Additionally, it covers methods for provisional restorations utilizing both direct and indirect techniques, along with specific applications in endodontics.