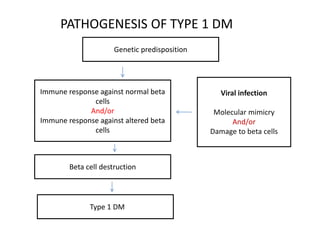
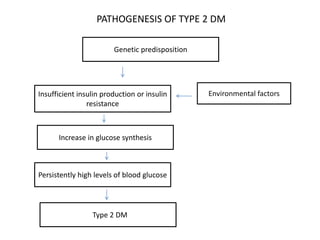
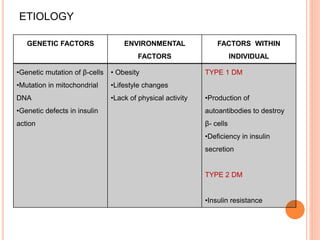
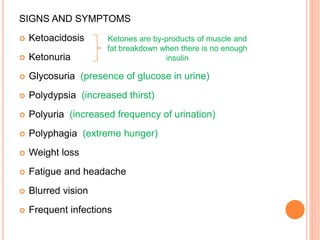
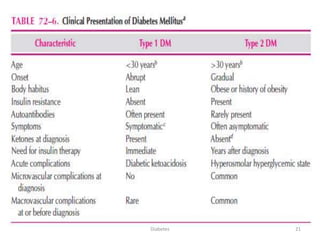
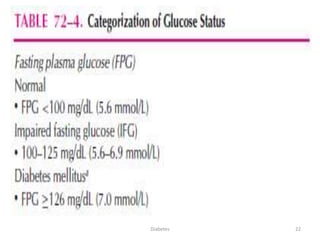
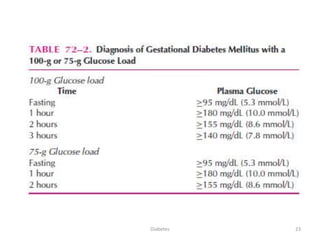
This document discusses diabetes pharmacotherapy. It provides an overview of the different types of diabetes, including type 1, type 2, gestational diabetes, and maturity onset diabetes of youth. It describes the pathogenesis and clinical presentation of type 1 and type 2 diabetes. The major components of diabetes treatment are diet, exercise, oral hypoglycemic medications, and insulin therapy. The document discusses the different types of insulin preparations, including their sources, structures, mechanisms of action, and uses. It provides guidance on calculating insulin doses and adjusting doses based on blood sugar levels.






























![DM lecture for c1 [Autosaved].ppt](https://cdn.slidesharecdn.com/ss_thumbnails/dmlectureforc1autosaved-220720190831-86418752-thumbnail.jpg?width=640&height=640&fit=bounds)

























































![Hypothalamus short notes on location, function and disorders by Dr. Neha [PT]...](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124142231-2b48143d-thumbnail.jpg?width=640&height=640&fit=bounds)