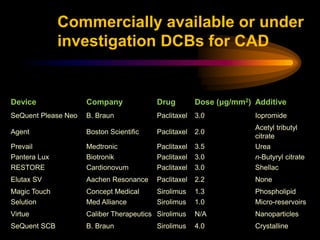
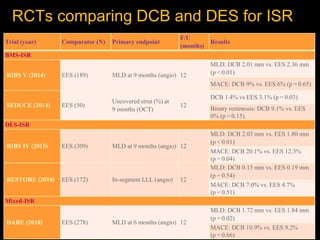
The document discusses the advantages and limitations of drug-coated balloons (DCBs) in interventional cardiology, highlighting their potential to treat vascular conditions without leaving permanent implants. It provides insights into various antiproliferative drugs used, efficacy in different lesion types, and the importance of optimal lesion preparation before DCB application. Additionally, ongoing studies are outlined to assess DCB performance in complex cases like bifurcation lesions and acute coronary syndromes.