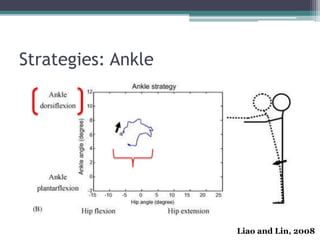
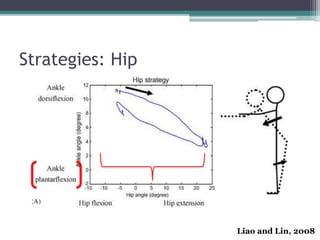
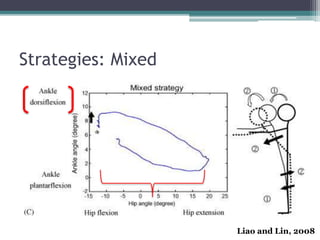
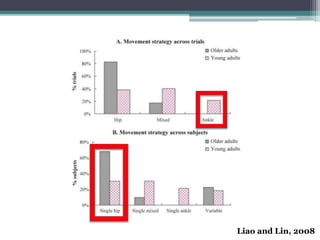
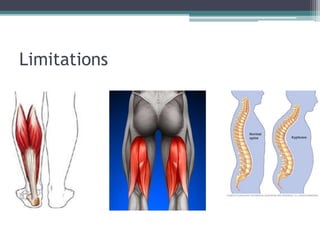
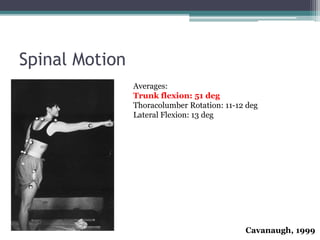
This document discusses forward reach, which requires moving the body's center of mass toward the front edge of the base of support in a controlled manner. It examines the strategies used in forward reach, including ankle, hip, and mixed strategies. Compensations like knee flexion and trunk rotation are also discussed. Limitations to forward reach due to factors like balance, strength, and health conditions like Parkinson's are covered.