This document discusses the key determinants for ascending stairs, including:
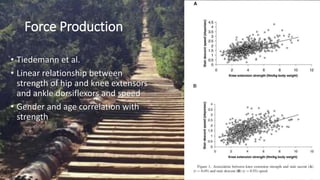
1. Lower extremity force production from muscles like the quadriceps and hip extensors is needed to move the center of mass over the base of support.
2. Dynamic postural stability during single limb stance is required for balance.
3. Lower extremity coordination of simultaneous hip and knee movement advances the center of mass.
4. Proper alignment of the torso, hip, knee and ankle is important.
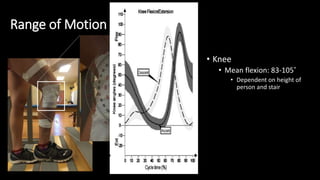
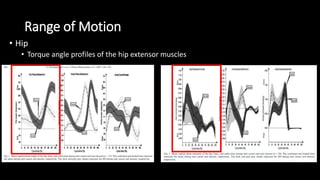
5. Sufficient range of motion at the hip, knee and ankle is necessary to complete the stair ascent task.


















































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)