Downloaded 14 times
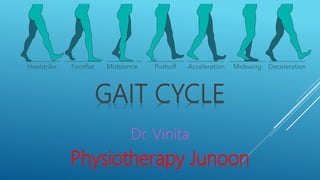




























The gait cycle document describes the phases and subdivisions of walking. It is broken down into: 1) initial contact, 2) opposite toe off, 3) heel rise, 4) opposite initial contact, 5) toe off, 6) feet adjacent, and 7) tibia vertical. The gait cycle is further subdivided into the swing phase and stance phase. Muscle activity varies throughout the gait cycle phases to control movement and provide stability and propulsion. Gait analysis is important for injury prevention, evaluating treatment effectiveness, sports performance optimization, and research on how different conditions affect walking.





































![GAIT and its different types[Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/gaitautosaved-240815185755-7939fafe-thumbnail.jpg?width=640&height=640&fit=bounds)











































