Downloaded 507 times


![~250 kb ~300 kb
t(2;5) ALK gene
breakpoint region
2p23 regionTelomere Centromere
3’ 5’
FISH Assay for ALK Rearrangement*
Break-apart FISH assay
for ALK-fusion genes1
ALK 29.3
EML4 42.3
ALK break-apart FISH assay
[Courtesy John Iafrate, Massachusetts General Hospital]
1
Shaw AT et al. J Clin Oncol
2009;27:4247–4253
q36.1
q36.3
q37.2
q34
q32.1
q32.3
q33.2
q31.3
q24.3
q24.1
q23.2
q22.2
q22.1
q21.2
q14.3
q14.1
q12.3
q12.1
p12
p13.2
p14
p16.1
p16.3
p22.1
p23.2
p22.3
p24.1
p24.3
p25.2
q36.1
q36.3
q37.2
q34
q32.1
q32.3
q33.2
q31.3
q24.3
q24.1
q23.2
q22.2
q22.1
q21.2
q14.3
q14.1
q12.3
q12.1
p12
p13.2
p14
p16.1
p16.3
p22.1
p23.2
p22.3
p24.1
p24.3
p25.2
Split signal
Non-split signal
*Assay is positive if rearrangements can be detected in ≥15% of cells
FISH = fluorescence in situ hybridization](https://image.slidesharecdn.com/sesionmedicosiraquiesxanitdrtrujillo-160428121717/85/Targeted-Therapy-in-Cancer-16-320.jpg)
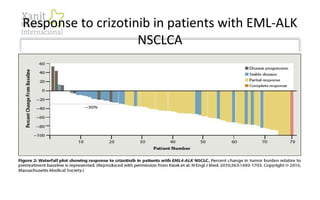
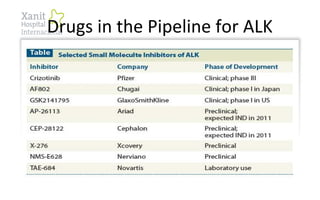
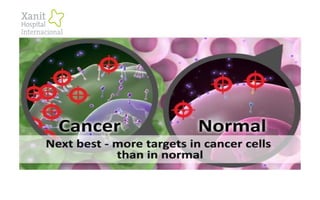
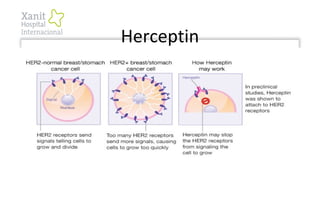
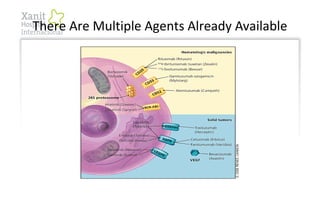

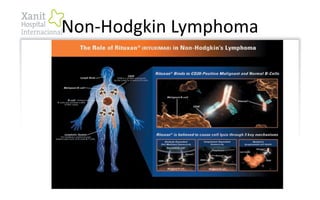
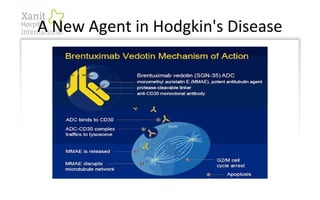
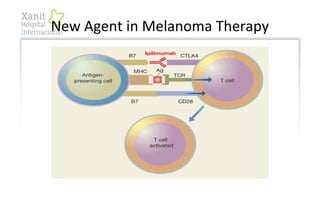
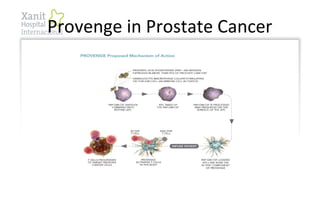


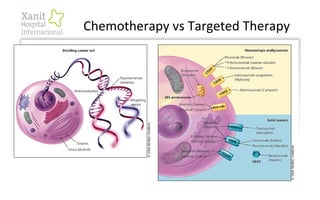
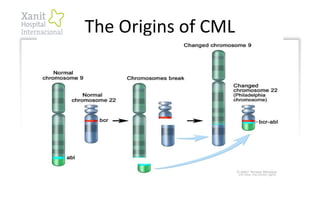
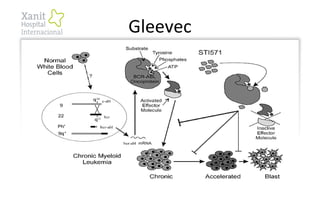
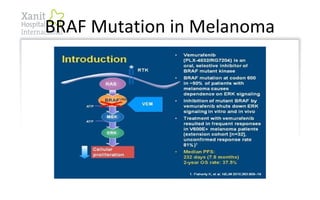
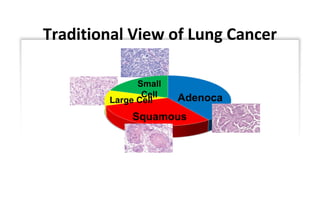
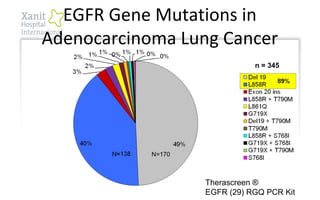
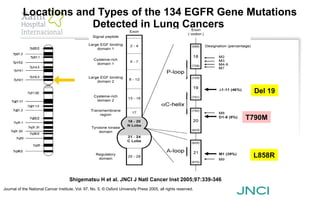
This document discusses targeted cancer therapy and provides several examples. It compares chemotherapy to targeted therapy, noting targeted therapy drugs inhibit more specific targets and include many oral agents. Examples discussed include Gleevec for CML targeting BCR-ABL fusion, EGFR mutations in lung cancer treated by drugs like Iressa, ALK rearrangements in lung cancer treated by crizotinib, BRAF mutations in melanoma treated by vemurafenib, and HER2-positive breast cancers treated by Herceptin. New immunotherapies and antibody-drug conjugates are also mentioned.































































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)
