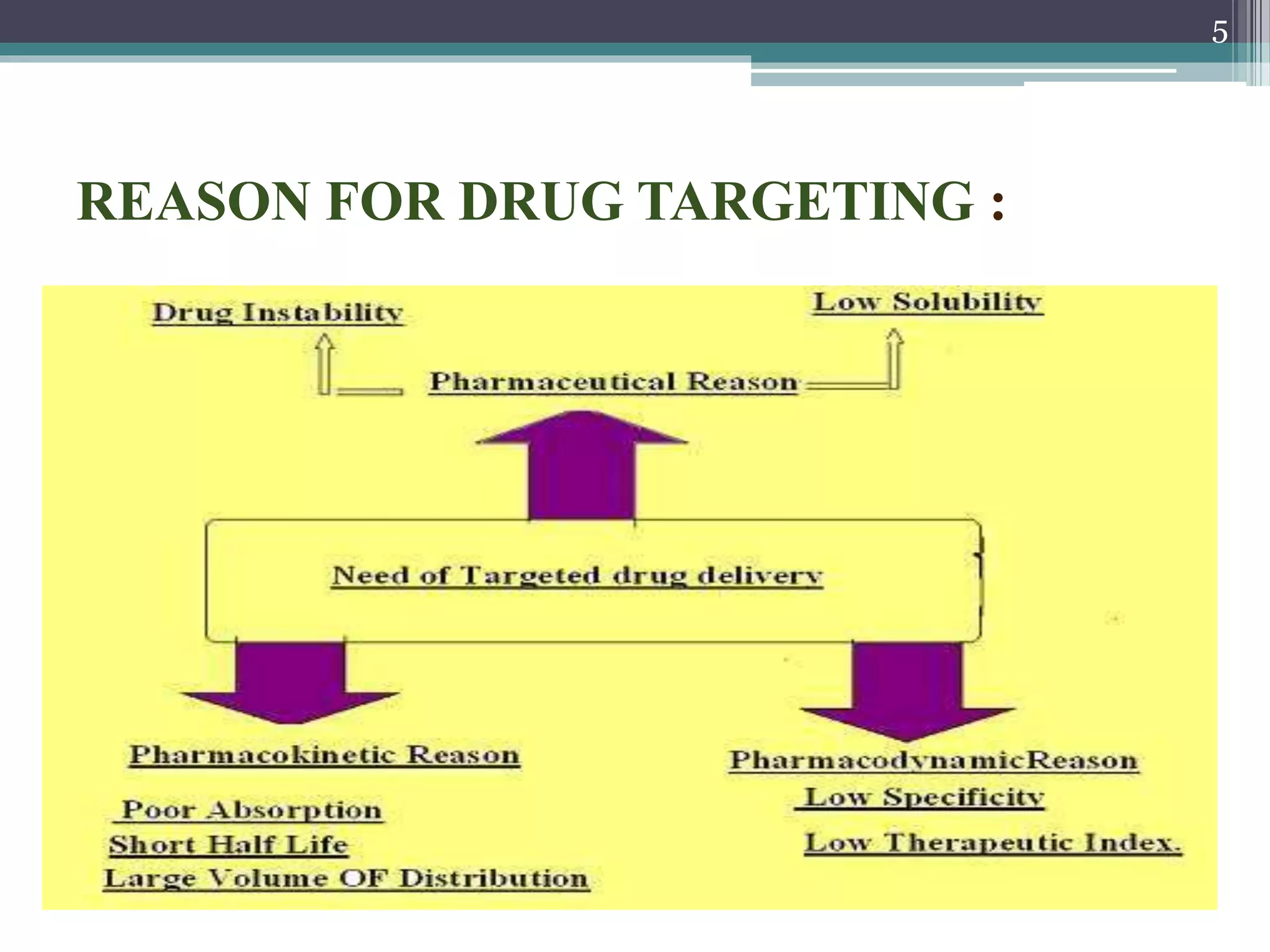
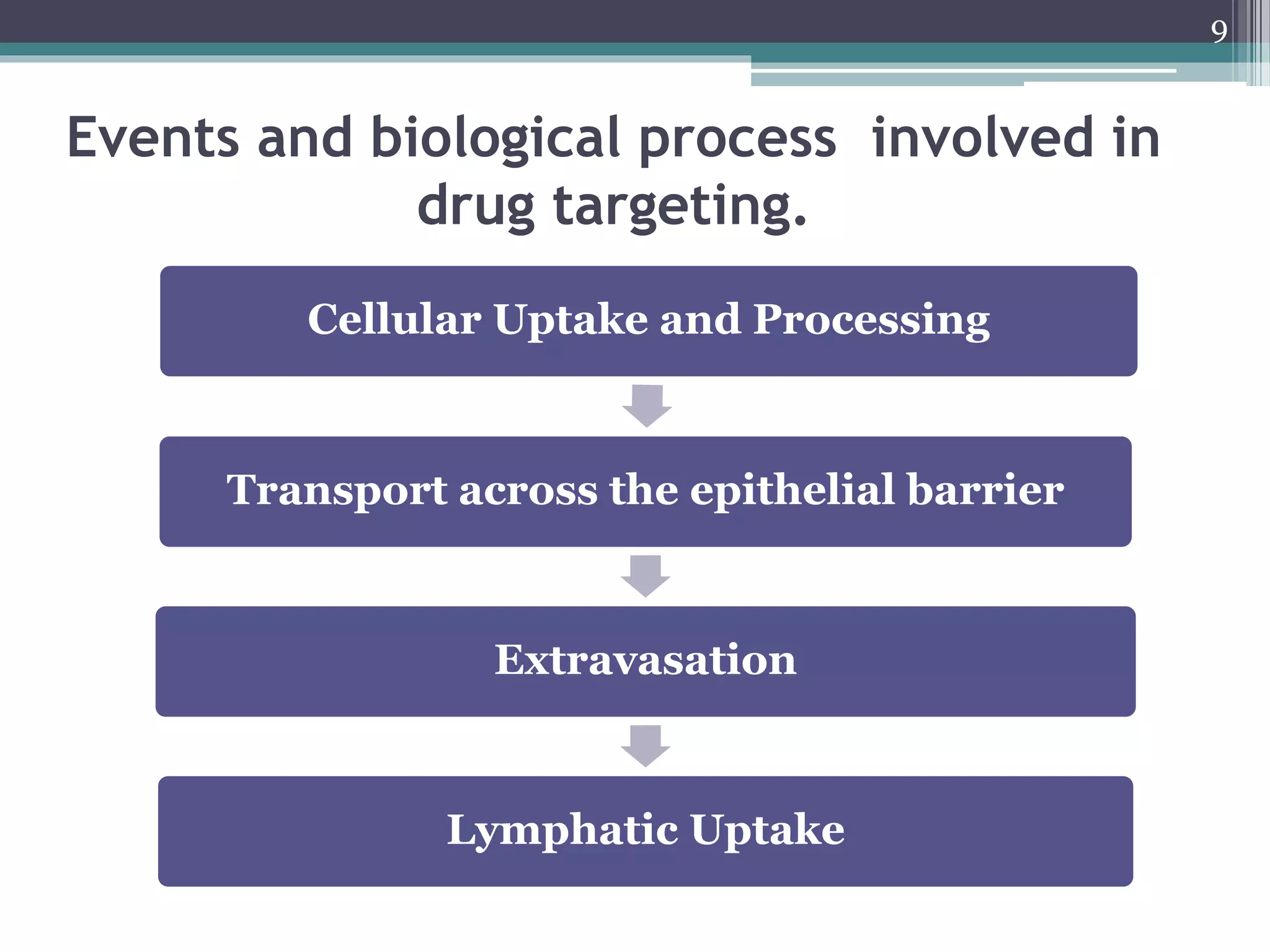
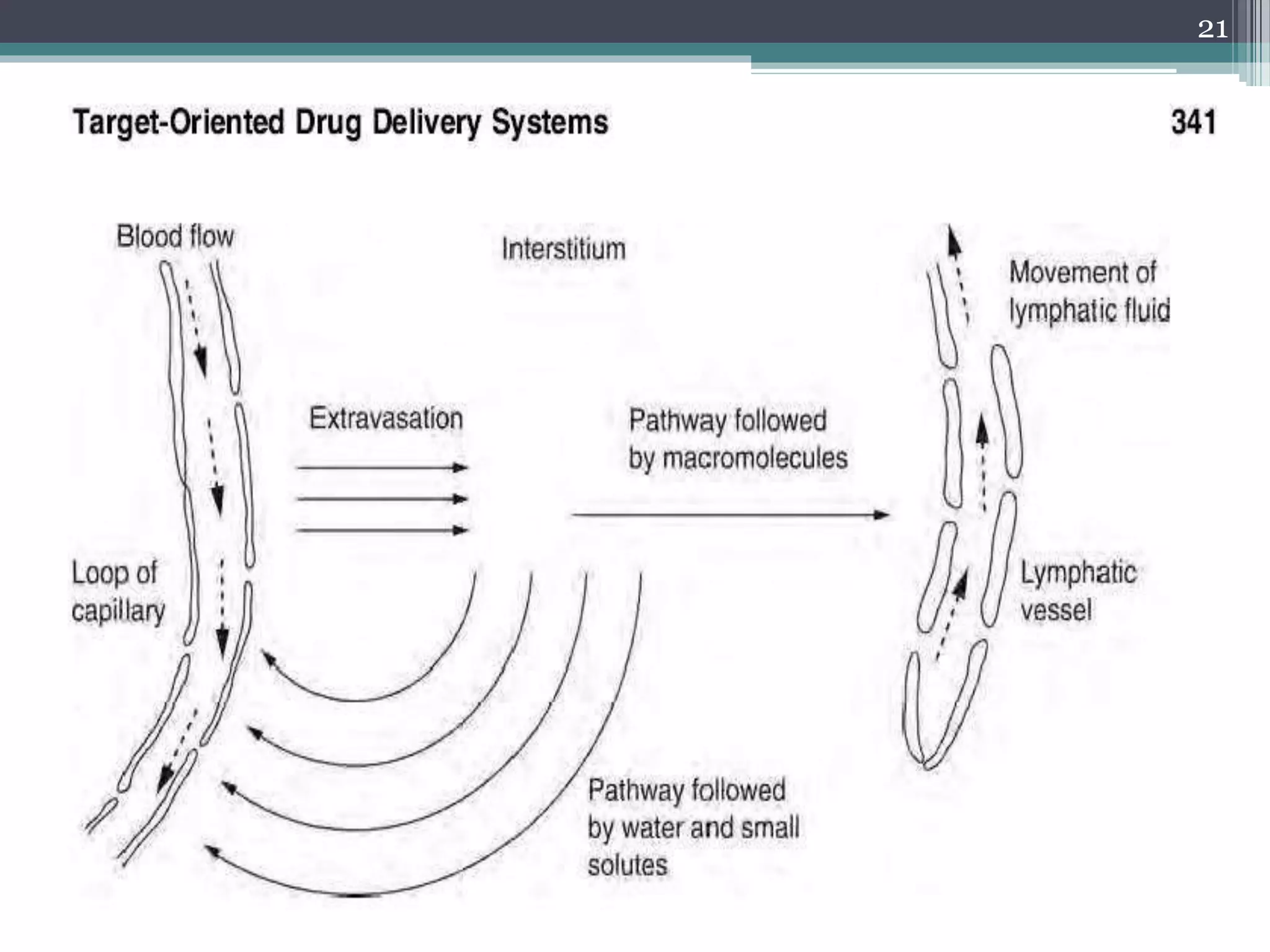
This document discusses targeted drug delivery systems. It begins by defining targeted drug delivery as selectively delivering medication only to its site of action to increase concentration there and reduce it elsewhere. This improves efficacy and reduces side effects. It then lists the ideal characteristics of targeted systems and the advantages they provide like reduced toxicity and dosage. The document outlines various carrier systems and the biological processes involved in cellular uptake, transport across barriers, extravasation into tissues, and lymphatic uptake. It concludes by describing different strategies for targeted delivery, including passive, active, and physical targeting approaches.