Download to read offline


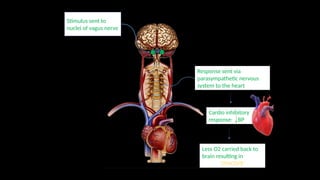
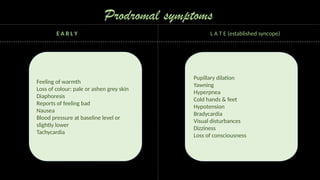
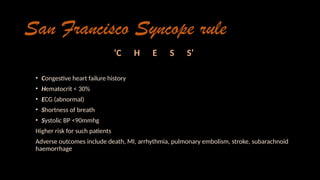
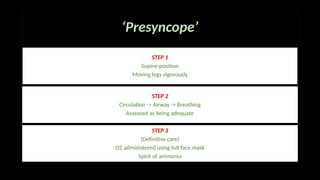

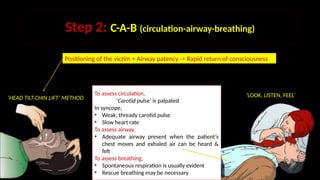






This presentation provides an overview of syncope, a common medical emergency in dental practice. Created during my internship, this presentation aims to educate dental students on the causes, symptoms, diagnosis and management of syncope with a focus on dental specific considerations.























































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)











