3
Definition
Greek word`SYNKOPTEIN` - to cut or break
Syncope is defined as transient loss of
consciousness due to reduced cerebral blood
flow.
A transient, self limited loss of consciousness
usually leading to falling. The onset of
syncope is relatively rapid, and the
subsequent recovery is spontaneous,
complete, and relatively prompt.
4.
4
Causes
A. Insuffficient pumpingaction of heart
-Arrythmia
-Structural cardiac disease
e.g. valvular disease,
obstructive cadiomyopathy
B. Insufficient vascular tone
-Autonomic failure
Primary e.g.multiple system atrophy
Secondary e.g. diabetic &
other neuropathy Drugs e.g.
antidepressants, beta blockers
C. Insufficient circulatory volume
- Hypovolemia e.g. Addisons disease, hemorrhage,
diuretics
D. Inappropriate neural control: reflex syncope
e.g. vasovagal, carotid sinus synd, micturation syncope
5.
5
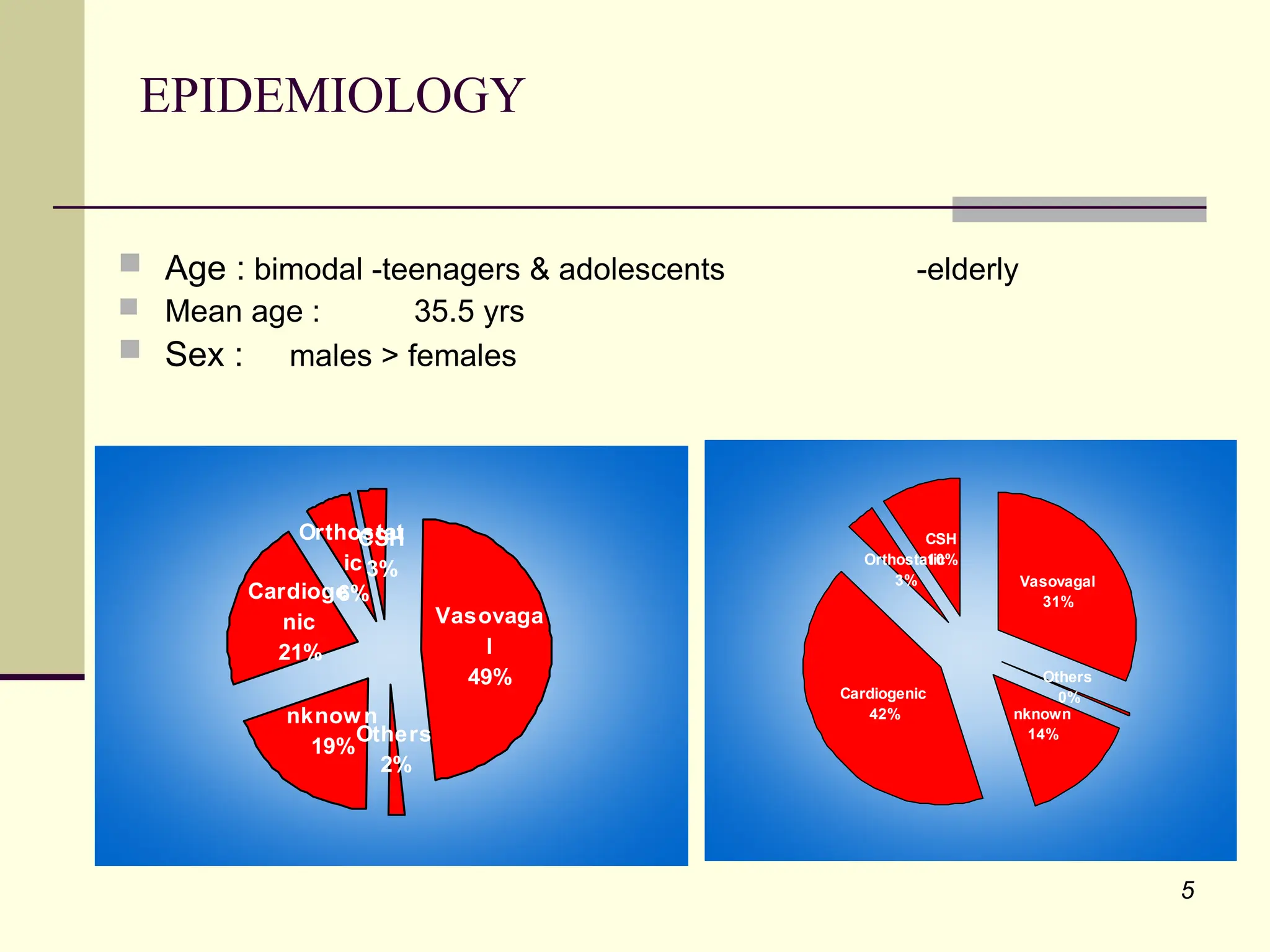
EPIDEMIOLOGY
Age :bimodal -teenagers & adolescents -elderly
Mean age : 35.5 yrs
Sex : males > females
Vasovaga
l
49%
Others
2%
nknown
19%
Cardioge
nic
21%
Orthostat
ic
6%
CSH
3% Vasovagal
31%
Others
0%
nknown
14%
Cardiogenic
42%
Orthostatic
3%
CSH
10%
6.
6
Predisposing factors
Psychogenicfactors
Fright
Anxiety
Emotional stress
Pain esp. unexpected &sudden
Sight of blood or surgical instrument
Non-psychogenic factors
Erect sitting or standing posture
Hunger or missed meal
Poor physical condition
Hot, humid, crowded enviornment
Exhaustion
7.
7
PATHOPHYSIOLOGY & CLINICALMANIFESTATIONS
ENGLE classified mechanisms producing syncope into 4 categories:
Inadequate delivery of blood / O2 to brain
ed cerebral metabolism.
General / local metabolic deficiencies
ed cerebral metabolism
Direct /Reflex effects on that part of CNS that
regulates consciousness and equilibrium.
Psychic mechanisms affecting levels of
consciousness with their respective mechanisms of
actions.
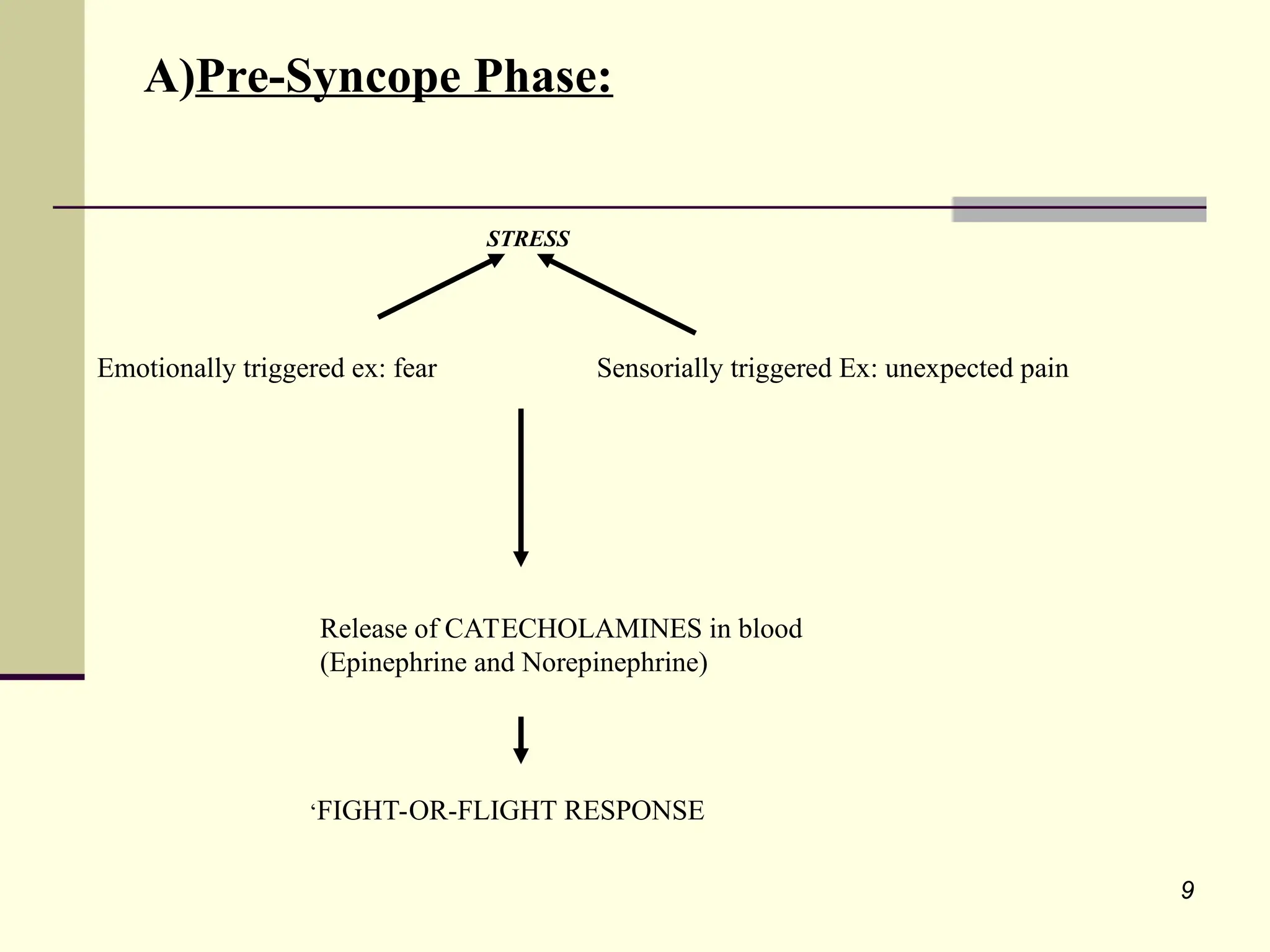
8.
8
PATHOPHYSIOLOGY & CLINICALMANIFESTATIONS OF
VASODEPRESSOR SYNCOPE:
Grouped into 3 different phases:
Pre-Syncope
Syncope
Post-Syncope
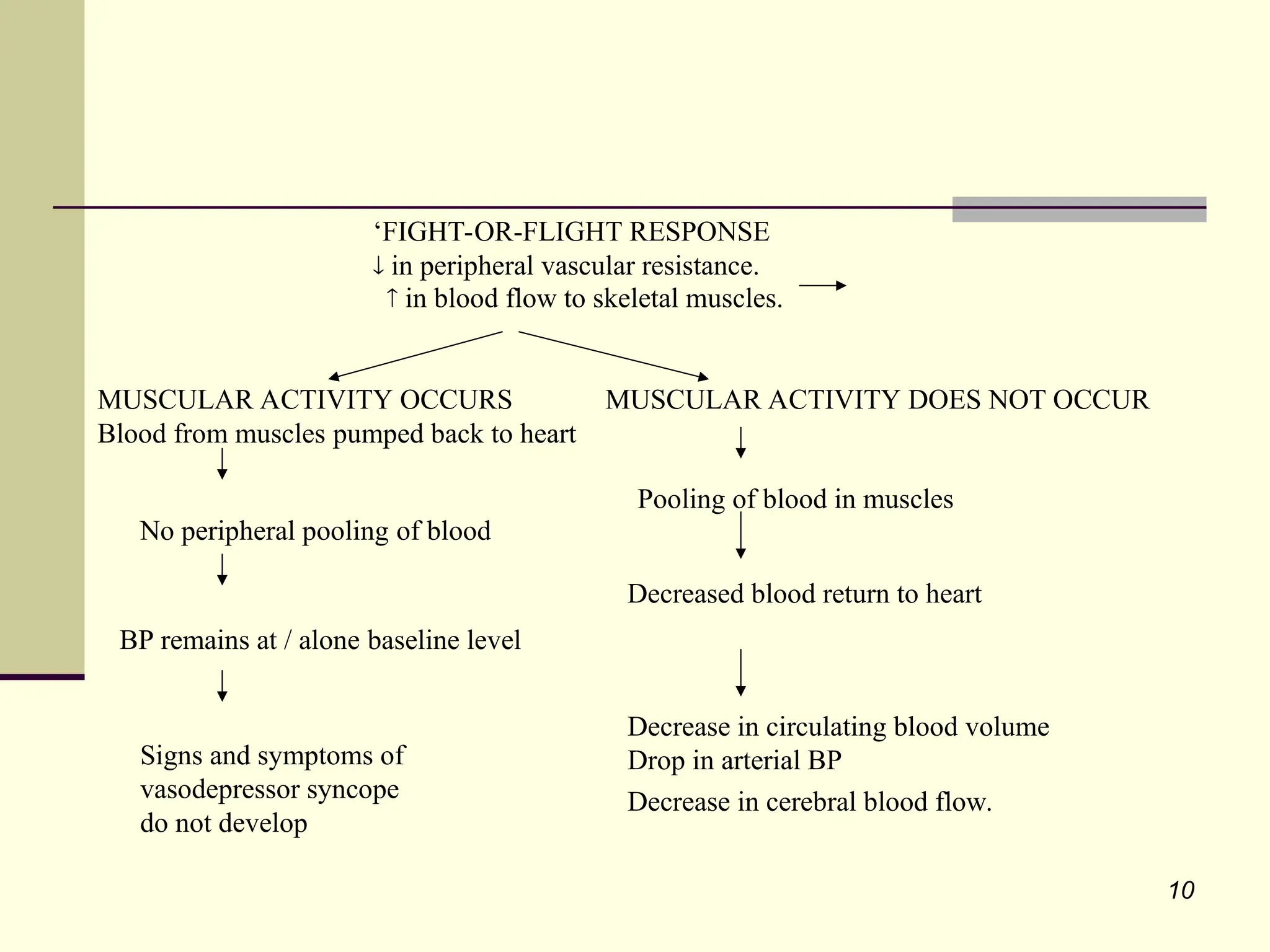
10
‘FIGHT-OR-FLIGHT RESPONSE
inperipheral vascular resistance.
in blood flow to skeletal muscles.
MUSCULAR ACTIVITY OCCURS MUSCULAR ACTIVITY DOES NOT OCCUR
Blood from muscles pumped back to heart
No peripheral pooling of blood
BP remains at / alone baseline level
Signs and symptoms of
vasodepressor syncope
do not develop
Pooling of blood in muscles
Decrease in circulating blood volume
Drop in arterial BP
Decrease in cerebral blood flow.
Decreased blood return to heart
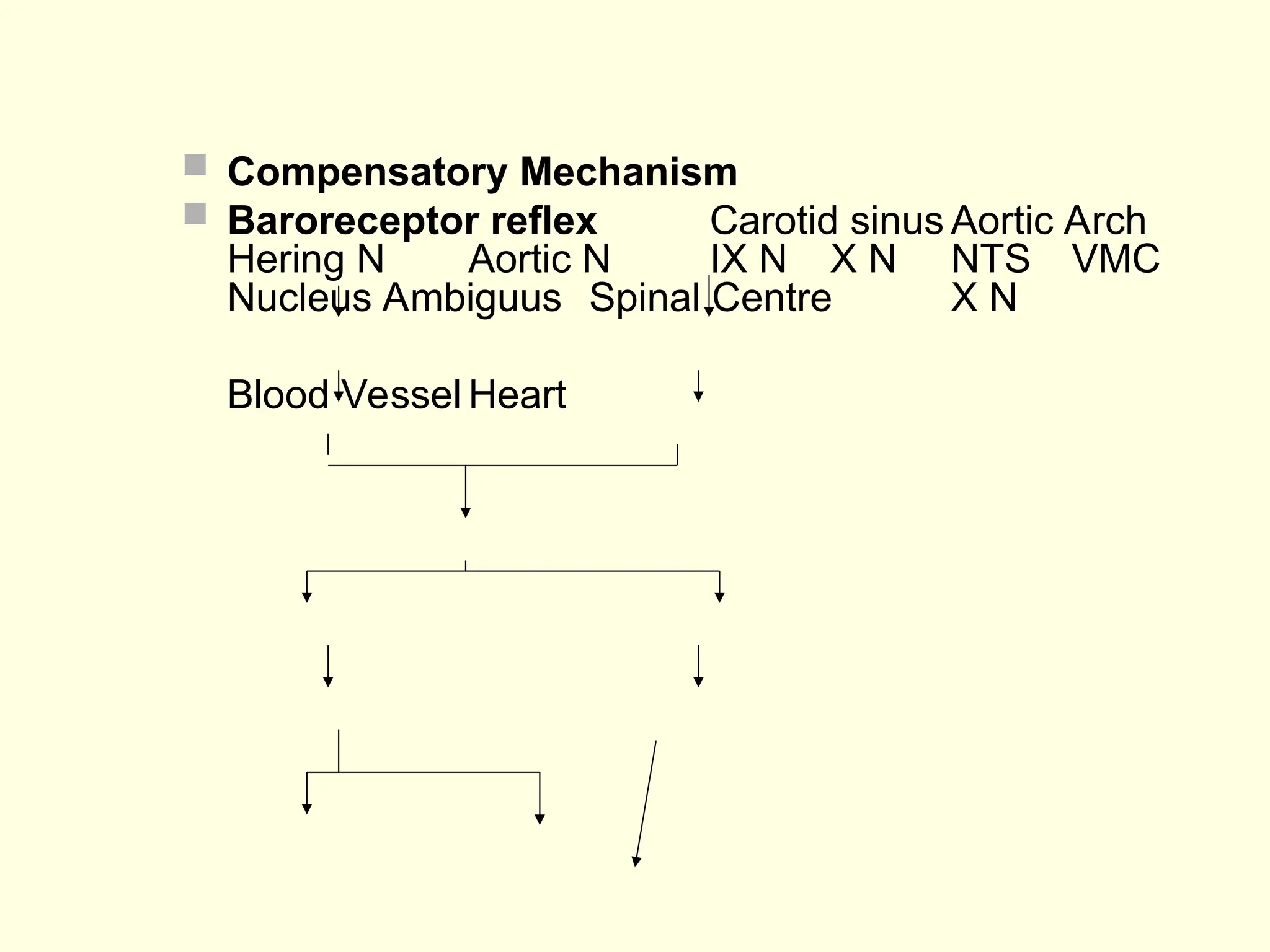
11.
Compensatory Mechanism
Baroreceptor reflex Carotid sinus Aortic Arch
Hering N Aortic N IX N X N NTS VMC
Nucleus Ambiguus Spinal Centre X N
Blood Vessel Heart
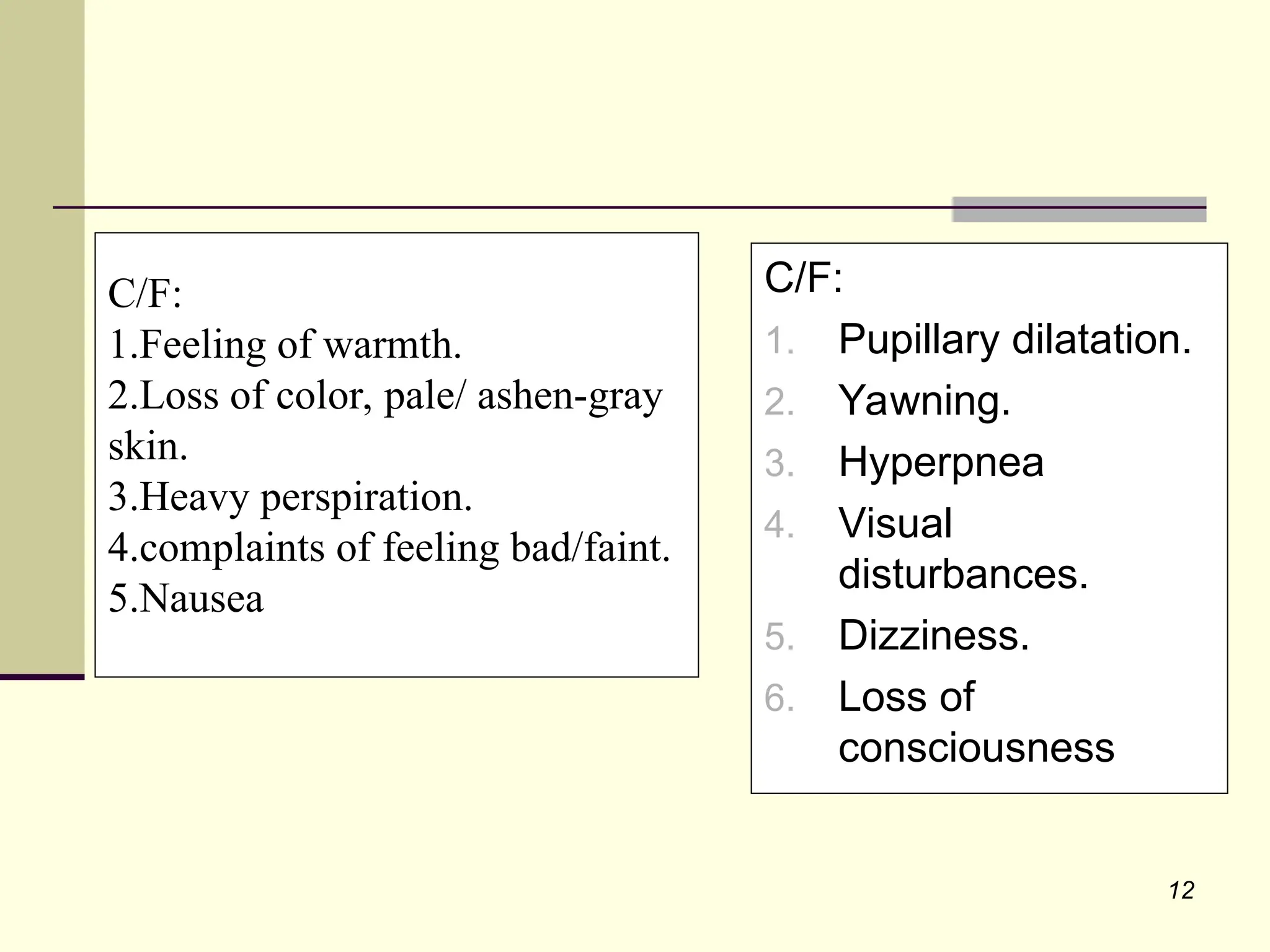
12.
12
C/F:
1.Feeling of warmth.
2.Lossof color, pale/ ashen-gray
skin.
3.Heavy perspiration.
4.complaints of feeling bad/faint.
5.Nausea
C/F:
1. Pupillary dilatation.
2. Yawning.
3. Hyperpnea
4. Visual
disturbances.
5. Dizziness.
6. Loss of
consciousness
13.
13
CRITICAL LEVELof cerebral blood flow for the
maintenance of consciousness.
30ml of blood / 100gm of brain tissue/ min.
NORMAL VALUE of blood flow is 50-55 ml/100gm/min.
- Equivalent to 70mm Hg SBP in normotensive patients.
- Reached with SBP>70mm Hg in patients with
atherosclerosis and high BP.
Human brain uses-
- 20% of total body O2
- 6.5% of total glucose consumed by body.
For a normal individual in supine position - Cerebral
blood flow – 750ml/min.
SYNCOPE PHASE
14.
14
Breathing -Irregular,jerky and gasping.
Dilation of pupils.
Cerebral ischemia -
Convulsive movements.
Muscular twitching of hands, legs or facial
muscles.
Bradycardia
BP
Pulse-weak and thready.
Loss of consciousness + Generalized muscular
relaxation.
Partial / complete airway obstruction
Clinical features:
15.
15
POST-SYNCOPE (RECOVERY) PHASE:
Farrecovery
Remove factor that precipitated episode.
Place victim in supine position with legs elevated
slightly.
Improvement in venous return to heart
Increase in blood flow to brain.
Cerebral blood flow exceeds critical level necessary for
consciousness.
16.
16
Pallor, nausea,weakness and sweating.
Disorientation and confusion.
Increase in arterial BP
Heart rate – returns to baseline level.
Pulse becomes stronger.
Tendency for patient to faint again may persist for many
hrs if patient assumes a sitting position or stands too soon.
Clinical features
17.
17
As soonas signs and symptoms are noted-
Terminate all procedures
Place patient in supine position with legs slightly elevated and back
of dental chair at 10° i.e. TRENDELENBURG POSITION
muscular movement aids in return of blood from periphery.
O2 if necessary (monitor vital signs)
Aromatic ammonia vapours crushed and held under patients nose.
Speeds recovery by direct stimulation of respiratory center
Note -no response BASIC LIFE SUPPORT
MANAGEMENT OF VASOVAGAL
SYNCOPE
18.
18
Position – Supinewith legs elevated.
Failure to lower patient in this position may cause death or permanent
neurological damage secondary to prolonged cerebral ischemia.
Pregnant woman in supine position
Gravid uterus presses on inferior vena cava.
CAVAL COMPRESSION / SUPINE HYPOTENSION SYNDROME
Acute fall in cardiac output
Recovery delayed
19.
19
Administration ofO2.
Monitoring of vital signs – BP, HR, Respiratory rate.
Performing additional procedures:
Loosening of tight clothes such as ties, collars,
bolts.
Ammonia vapours – stimulates both breathing
and muscular movements.
Cold towel over patient’s forehead.
Blanket if patient is shivering.
If bradycardia persists – Atropine (i.v./i.m.)
Reassure patient.
DEFINITITIVE CARE
20.
20
POST-SYNCOPE STAGE
Determineprecipitating factors and prevent
recurrence of syncope.
No dental treatment for next 24 hours.
Arrange for patient to be escorted home.
21.
21
DRUGS USED INMANAGEMENT OF VASOVAGAL SYNCOPE
Atropine
given if bradycardia persists
competitively inhibits acetyl-choline
Dose - 0.5 mg i.v./i.m./ s.c.
Dextrose – Restores blood glucose levels.
Dose – 1-2 ampules of 5% dextrose i.v.
Midoprine HCl – Vasopressor
1-agonist
acts on receptor of arteriolar and venous vasculature
in vascular tone
in BP
Dose – 10mg tid
Beta blockers – propranolol, atenolol