Downloaded 762 times


![ HTWU does not have TN manufacturing facility
PN ordered from HQE 2, KK – only Monday to Thursday.
Take around 2 days to receive the TPN bags (May also be on weekend)
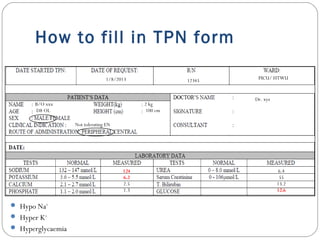
Incomplete TN form
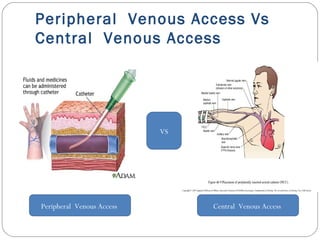
Central line/ peripheral line?
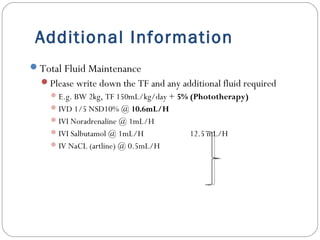
Fluid maintenance? [Total Fluid (TF)]
PN regimen?
Crucial info for TN administration
Centrally? Peripherally?
Content of PN?
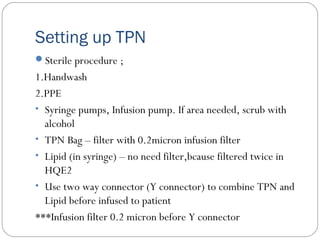
Aseptic Technique?](https://image.slidesharecdn.com/paedspnedited-151001042415-lva1-app6891/85/Pediatric-Parenteral-Nutrition-59-320.jpg)



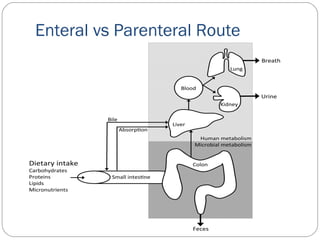
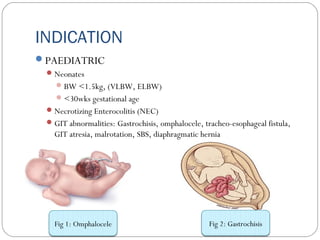
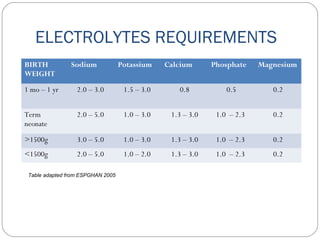
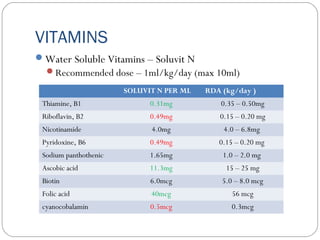
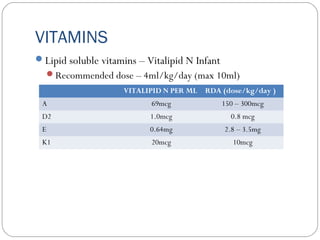
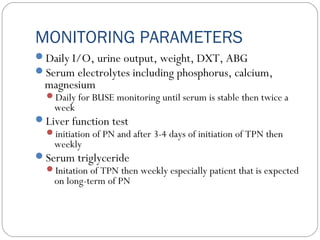
This document provides information on pediatric parenteral nutrition. It discusses enteral versus parenteral routes of feeding and notes that whenever possible, the enteral route is preferred. The document outlines indications for total parenteral nutrition (TPN) in pediatric patients, including very low birth weight neonates and infants with gastrointestinal abnormalities. It also covers assessments needed for nutrition support, including growth curves and caloric requirements. The document discusses macronutrient needs for carbohydrates, proteins, and lipids in pediatric TPN. It concludes with information on electrolyte and micronutrient requirements and considerations for administering and monitoring pediatric parenteral nutrition.



















































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)












