Downloaded 308 times




















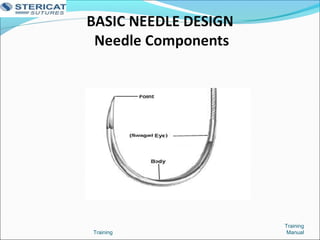
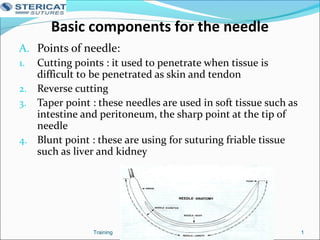

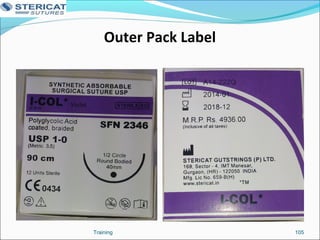
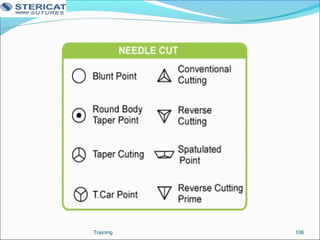






The document provides information about Stericat, a suture manufacturing company in India. It discusses Stericat's mission and vision of being a leading suture company offering high quality products at reasonable prices. It then details Stericat's 30 years of experience in suture manufacturing and its certifications. The rest of the document showcases Stericat's manufacturing facility and processes, product varieties, presence in hospitals, and marketing offices. It also includes sections on the history of sutures, classification of sutures, needles, labeling, and knot tying and suturing techniques.



































































