
![EMA on biomarkersDecember 2005: EMEA biomarkers workshops with academia and healthcare professionalsDecember 2006: EMEA biomarkers workshops with the EFPIA and with all stakeholders July 2008: First EMEA-FDA joint biomarkers qualification processSource: Human Medicines - Medicines and Emerging Science - Biomarkers [Internet]. [cited 2010 Jun 3]; Available from: http://www.ema.europa.eu/htms/human/mes/biomarkers.htm](https://image.slidesharecdn.com/surrogateendpoints-100611051757-phpapp01/85/Surrogate-endpoints-a-regulatory-review-7-320.jpg)
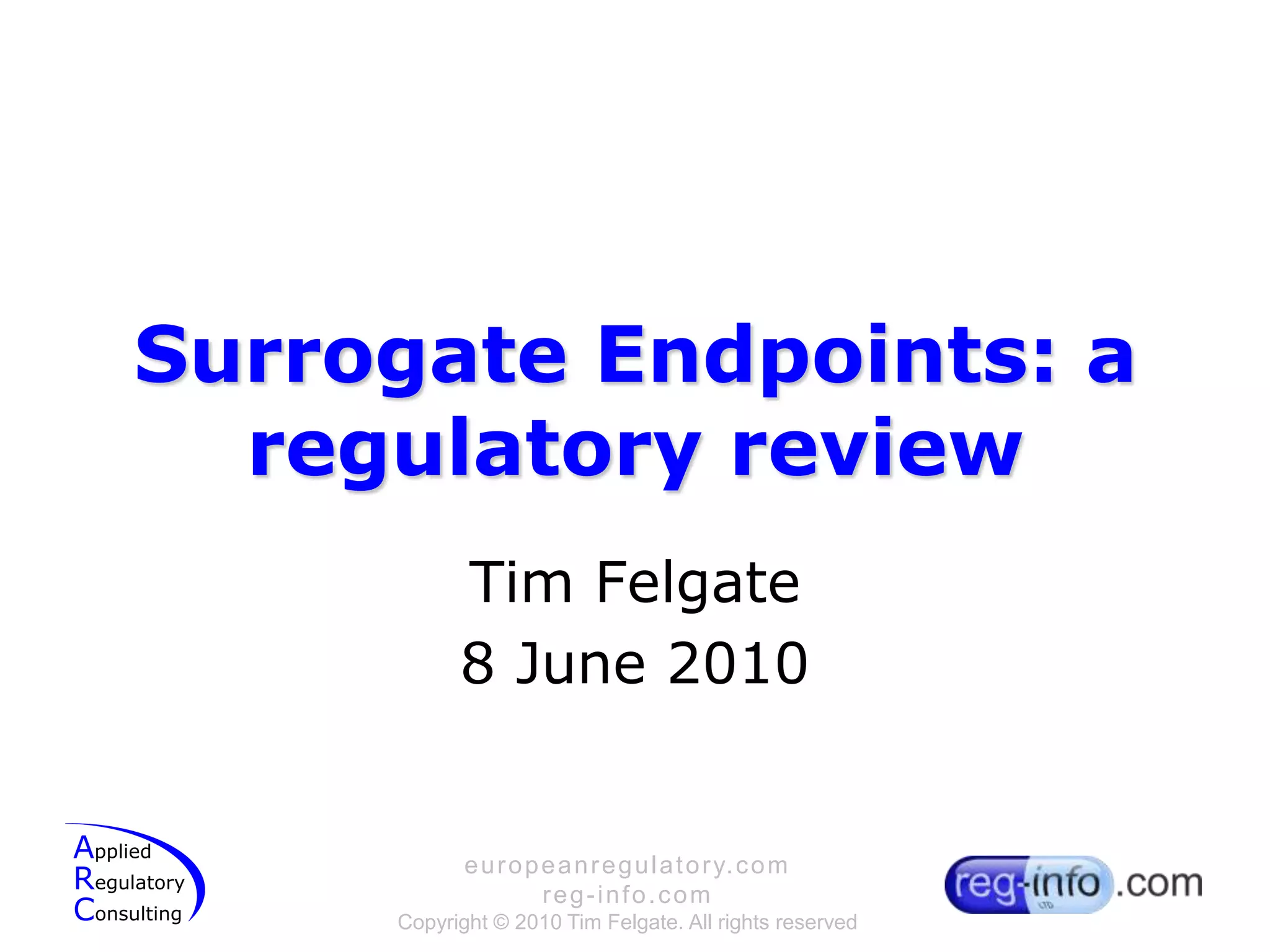
![The ENHANCE trial:MHRA statement (2008)The results showed that patients assigned simvastatin plus ezetimibehad significantly lower mean LDL cholesterol than did those assigned simvastatinplus placebo at the end of the study (3·65 mmol/L [SD 1·36] vs 4·98 mmol/L [SD 1·56]; difference between groups 16·5%, p<0·01). However, mean change in intima–media thickness of the carotid artery did not differ significantly between groups (0·0111 mm [SE 0·0038] vs 0·0058 mm [SE 0.0037], respectively, p=0·29).To date, no data from large clinical outcomes trials are available for ezetimibe. The ongoing IMPROVE-IT trial (IMProved Reduction of Outcomes: VytorinEfficacy International Trial) is evaluating the clinical benefit—in terms of cardiovascular morbidity and mortality—of ezetimibe combined with simvastatin compared with simvastatinalone in about 10 000 patients with acute coronary syndromes. However, the results are not expected to be available in the next 4 years.The MHRA, together with other regulatory agencies in the European Union, is currently reviewing the results of the ENHANCE trial to establish their clinical significance and potential effect on the balance of benefits and risks for ezetimibe. We will inform healthcare professionals of any changes to prescribing advice as soon as these reviews have been completed.A couple of useful links: http://j.mp/cjyk5p; http://j.mp/aeOS47](https://image.slidesharecdn.com/surrogateendpoints-100611051757-phpapp01/85/Surrogate-endpoints-a-regulatory-review-17-320.jpg)


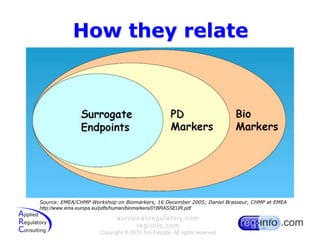
Surrogate endpoints are biomarkers intended to substitute for clinical endpoints and predict clinical benefit from a treatment. Regulatory agencies provide guidance on using surrogate endpoints for drug approval. The EMA and FDA may approve drugs based on surrogate endpoints that are reasonably likely to predict clinical benefit, but require post-marketing studies to verify the clinical benefit. The EMA guidance documents discuss considerations for various disease areas, noting surrogate endpoints must be validated and their relationship to clinical outcomes understood to support drug approval.













































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)



