Indication
Coronary arterydisease
Valvular heart disease
First line test in patients with baseline ECG
abnormalities – that preclude interpretation of
exercise ECG
3.
CORONARY ARTERY DISEASE
Detection of CAD
Localisation of coronary artery lesion
Post MI- Risk assessment
After revascularisation
Viability assessment
Preoperative evaluation
4.
PHYSIOLOGICAL BASIS
• Causalrelationship between induced myocardial ischemia
and left ventricular wall motion abnormalities
• Stress Increased HR and contractility increased
myocardial blood flow hypercontractile response with
increased EF
5.
• Most commonapplication- Detection of flow limiting
stenosis
• Based on sequence of events - Ischemic cascade
• Normal coronary arteries adapt to stress by coronary
vasodilatation (coronary flow reserve)—to meet the
increased oxygen demand
• In the presence of flow limiting coronary stenosis-
coronary flow reserve is impaired- resulting in ischemic
cascade
7.
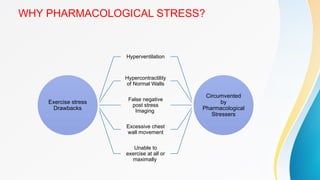
WHY PHARMACOLOGICAL STRESS?
Exercisestress
Drawbacks
Hyperventilation
Hypercontractility
of Normal Walls
False negative
post stress
Imaging
Excessive chest
wall movement
Unable to
exercise at all or
maximally
Circumvented
by
Pharmacological
Stressers
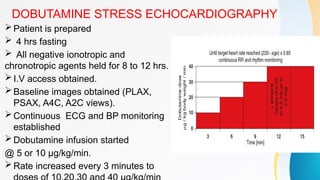
DOBUTAMINE STRESS ECHOCARDIOGRAPHY
Patientis prepared
4 hrs fasting
All negative ionotropic and
chronotropic agents held for 8 to 12 hrs.
I.V access obtained.
Baseline images obtained (PLAX,
PSAX, A4C, A2C views).
Continuous ECG and BP monitoring
established
Dobutamine infusion started
@ 5 or 10 µg/kg/min.
Rate increased every 3 minutes to
11.
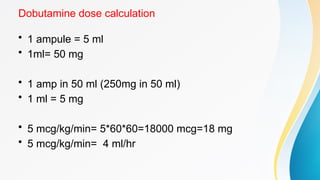
Dobutamine dose calculation
•1 ampule = 5 ml
• 1ml= 50 mg
• 1 amp in 50 ml (250mg in 50 ml)
• 1 ml = 5 mg
• 5 mcg/kg/min= 5*60*60=18000 mcg=18 mg
• 5 mcg/kg/min= 4 ml/hr
12.
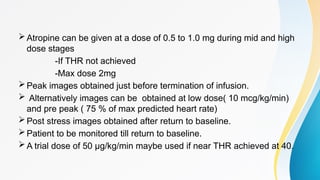
Atropine can begiven at a dose of 0.5 to 1.0 mg during mid and high
dose stages
-If THR not achieved
-Max dose 2mg
Peak images obtained just before termination of infusion.
Alternatively images can be obtained at low dose( 10 mcg/kg/min)
and pre peak ( 75 % of max predicted heart rate)
Post stress images obtained after return to baseline.
Patient to be monitored till return to baseline.
A trial dose of 50 µg/kg/min maybe used if near THR achieved at 40.
13.
Handgrip exercise
• Handgripmay be used as an adjunct to exercise or
dobutamine stress echocardiography
• During the last stage of exercise or dobutamine infusion
and 30 seconds before acquiring the peak exercise
images, patients are asked to exert a sustained grip on a
ball
14.
INDICATIONS TO TERMINATEDOBUTAMINE
INFUSION DURING STRESS ECHO
• 1.Exceeding THR of 85% age predicted maximum.
• 2.Development of significant angina.
• 3.Recognition of a new wall motion abnormality.
• 4.A decrease in SBP > 20 mm Hg from baseline.
• 5.Sustained or symptomatic arrhythmias.
• 6.Limiting side effects or symptoms.
• 7.Severe HTN ( > 220/120 mmHG)
15.
SAFETY
• Short t1/2(2 minutes) -- induced ischemia readily reversed
by termination of infusion.
• Severe cases - short acting i.v β Blocker- Esmolol or
Metoprolol can be used
• Overall rate of life threatening events- 1/1000
• Frequent complication observed - Non sustained VT(2-
3% %), AF(0.5 - 1%), VF(0.04%).
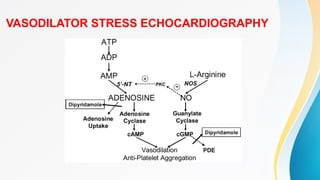
VASODILATOR STRESS ECHOCARDIOGRAPHY
•Dipyridamole is administered at up to 0.84 mg/kg in two separate
infusions: 0.56 mg/kg over four minutes ("standard dose"), followed
by four minutes of no dose and 0.28 mg/kg is given over two
minutes.
• Additional doses may be required in patients receiving beta blockers
and those with single vessel disease.
• If no endpoint is reached following the second infusion (total of 0.84
mg/kg), then atropine (doses of 0.25 mg, up to a maximum of 1 mg)
may be administered.
• Peak stress images are obtained at 4 and 6 minutes.
18.
• Adenosine istypically infused at a maximum dose of 140
mcg/kg/minute over six minutes.
• Imaging is performed prior to and after starting adenosine infusion.
• Peak stress images are obtained at 3 and 6 minutes
• Adenosine is a shorteracting agent employed for myocardial
perfusion contrast echocardiography
• Vasodilator stress may be better suited for perfusion than wall motion
analysis
• Contraindicated in patients with reactive airway obstruction or
significant conduction defects
• Not widely used
• Ergonovine is used to provoke coronary vasospasm in patients with
suspected vasospastic angina
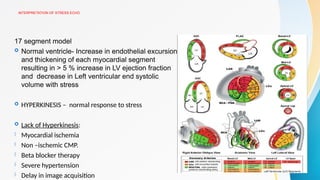
INTERPRETATION OF STRESSECHO
17 segment model
Normal ventricle- Increase in endothelial excursion
and thickening of each myocardial segment
resulting in > 5 % increase in LV ejection fraction
and decrease in Left ventricular end systolic
volume with stress
HYPERKINESIS – normal response to stress
Lack of Hyperkinesis:
- Myocardial ischemia
- Non –ischemic CMP.
- Beta blocker therapy
- Severe hypertension
- Delay in image acquisition
21.
Volume response
Decreasein ESV and EDV – Normal response
25-30% decrease in ESV and EDV is the normal response.
An abnormal volume response is defined as an increase in volume from rest to
stress of > 17%.
22.
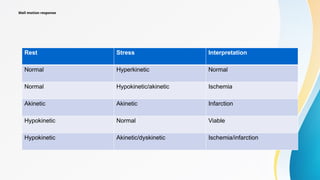
Wall motion response
RestStress Interpretation
Normal Hyperkinetic Normal
Normal Hypokinetic/akinetic Ischemia
Akinetic Akinetic Infarction
Hypokinetic Normal Viable
Hypokinetic Akinetic/dyskinetic Ischemia/infarction
23.
ASSESMENT OF MYOCARDIALVIABILITY
The term viable refers to myocardium that has the potential
for functional recovery.
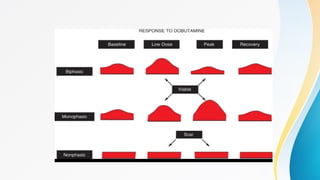
The BIPHASIC RESPONSE -- augmentation at low dose
followed by deterioration at higher doses is most predictive
of the capacity for functional recovery.
Any improvement in wall motion abnormality by at least
one grade in two or more segments during stress is likely
to signify viability.
25.
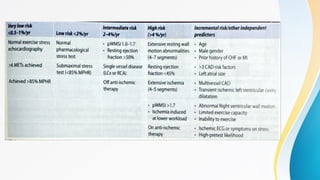
RISK STRATIFICATION
• Patientswho complete normal exercise or pharmacologic
stress echo (reaching good exercise capacity and the
target heart rate)-- the risk for cardiac events is very low
and close to that of a normal population
• <1%/ year for exercise and <2% / yr for pharmacologic
tests
27.
STRESS ECHO AFTERMI
Used both to identify high and low risk subsets and to
predict the location and extent of CAD.
The goal is to identify ischemia at a distance positive
finding would be detection of a new WMA remote from the
site of previous infarction.
Inducible ischemia is a powerful indicator of high risk and
suggests the need for further evaluation.
28.
Preoperative Risk Assessment
Most studies used dobutamine stress.
Mainly before major peripheral vascular surgery and therefore
included patients who frequently are unable to exercise.
In this high-risk subset, the presence or absence of an inducible
WMA has been the most potent determinant of relative risk.
The absence of an inducible wall motion abnormality confers a
very favorable prognosis, with a negative predictive value of
93% to 100%.
29.
STRESS ECHO INVALVULAR HEART DISEASE
• The principal role of stress testing is to unmask symptoms
or abnormal blood pressure responses in patients who
appear to be asymptomatic and to assess myocardial or
contractile reserve
30.
LOW FLOW LOWGRADIENT AS
• DSE can be used to assess both the true severity of AS and the
amount of LV contractile reserve
• Dobutamine is infused in graded doses from 5 to 20 μg/kg/min
• spectral Doppler of the LVOT and CW Doppler across the aortic
valve
• SV is calculated from VTI LVOT.
• An increase of 20% or higher in SV is indicative of significant
contractile reserve.
• The test is indeterminate if little or no augmentation of LV
function takes place (no contractile reserve, or SV <20%).
31.
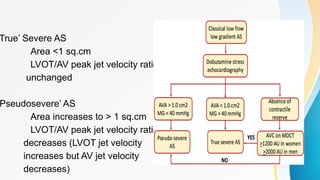
True’ Severe AS
Area<1 sq.cm
LVOT/AV peak jet velocity ratio
unchanged
Pseudosevere’ AS
Area increases to > 1 sq.cm
LVOT/AV peak jet velocity ratio
decreases (LVOT jet velocity
increases but AV jet velocity
decreases)
32.
MITRAL STENOSIS
• Patientswith mitral stenosis (MS) may have severe
exertional symptoms despite relatively modest gradients
on the resting echocardiogram.
• Conversely, sedentary patients with severe MS may be
relatively asymptomatic because they are inactive.
• Valve gradients -- dependent on the flow rate and heart
rate
• A rise in the mean transmitral pressure gradient greater
than 15 mm Hg or an increase in calculated pulmonary
artery systolic pressure greater than 60 mm Hg is
correlated with significant MS and consider BMV
33.
In asymptomatic patientswith severe MS (mean gradient >10
mm Hg and mitral valve area [MVA] <1.5 cm2
) or
Symptomaticpatients with moderate MS (mean gradient of 5
to 10 mm Hg andMVA > 1.5 cm2
)
34.
MITRAL REGURGITATION
• DSEmay be helpful in cases where ischemic heart disease is
suspected as a cause of MR.
• It can help identify viable myocardium and assess the impact of
ischemia on MR severity.
• In chronic severe MR, even if the LVEF is preserved, demonstration of
a rise in PASP> 60mmHg with stress and reduced LV contractile
reserve -- indications for mitral valve surgery.
35.
Other indications
• Hypertrophiccardiomyopathy – exercise can bring out
latent gradients and assess symptoms such as syncope -
Class IIA
• Latent Diastolic dysfunction
• Prosthetic valve gradient
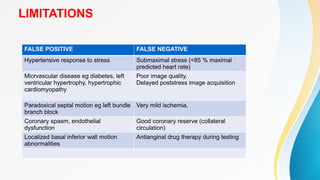
LIMITATIONS
FALSE POSITIVE FALSENEGATIVE
Hypertensive response to stress Submaximal stress (<85 % maximal
predicted heart rate)
Micrvascular disease eg diabetes, left
ventricular hypertrophy, hypertrophic
cardiomyopathy
Poor image quality,
Delayed poststress image acquisition
Paradoxical septal motion eg left bundle
branch block
Very mild ischemia,
Coronary spasm, endothelial
dysfunction
Good coronary reserve (collateral
circulation)
Localized basal inferior wall motion
abnormalities
Antianginal drug therapy during testing
39.
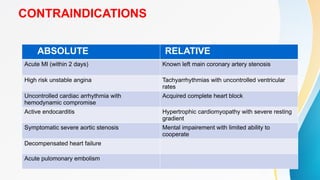
CONTRAINDICATIONS
ABSOLUTE RELATIVE
Acute MI(within 2 days) Known left main coronary artery stenosis
High risk unstable angina Tachyarrhythmias with uncontrolled ventricular
rates
Uncontrolled cardiac arrhythmia with
hemodynamic compromise
Acquired complete heart block
Active endocarditis Hypertrophic cardiomyopathy with severe resting
gradient
Symptomatic severe aortic stenosis Mental impairement with limited ability to
cooperate
Decompensated heart failure
Acute pulomonary embolism
#4 Systolic wall thickening Endocardial excursion Decrease in End SystolicVolume
#5 THE SEVERITY AND EXTENT OF WALL MOTION ABNORMALITIES DEPENDS ON SEVEROTY OF STENOSIS , LEVEL OF STRESS, CORONARY FLOW RESERVE AND COLLATERA;L CIRCUL;ATION
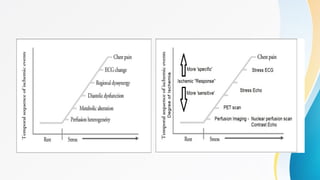
#6 in both graphs it shows that how ischemic cascade progresses and highlight how to diagnose it at different stages
when there is stress
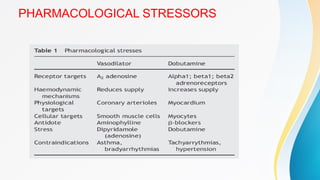
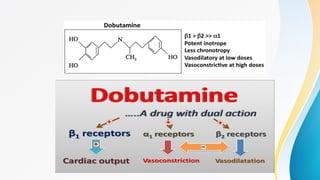
#8 DOBUTAMINE IS PREFFERED AS IT IS MORE LIKELY TO PROVOKE ISCHEMIA AS COMPARED TO OTHER AGENTS
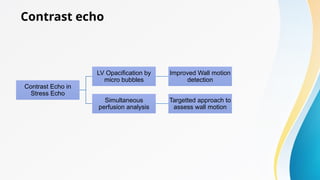
#10 a quad screen format is used to assess for simultaneous assessment
#13 The hand grip response reliably increases heart rate by increasing afterload
#18 Adenosin can also used in lbbb patients where there is difficulty in interpretation of images after dobutamine stress echo in tachycardia
Methylxanthines such as theophylline or caffeine, block adenosine binding due to antagonistic action at A2A receptors and can reduce the coronary vasodilation effects of adenosine. Therefore, it is recommended to discontinue consumption of caffeine-containing medications, foods, or beverages for at least 12 hours and ideally 24 hours before adenosine stress testing
#19 If endocardial resolution is poor in 2 or more segments- IV echo contrast enhancement
#22 akinetic no wall motion and thickening
hypokinesia is reduced wall motion and thickening
#24 During testing segements are compared at rest , low dose , peak dose and recovery Row 1 biphasic describes an initial improvement in heart muscle function and then at peak doses decline in heart muscle functions it indicates the hibernating myocardium which is potentially viable with ischemia and can recover after revascularisation
in contrast monophasic response therse is improvement in heart muscle function at low and peak doses indicating viable myocardium without ischemia
third is non phasic in this it remains throughout indicating non viable , scar tissue
#26 patients with intermediate riskof cardiac events can be maanaged medically
patients with high risk should be considered for coronary revascularisation
#30
Anatomically severe AS and LV systolic dysfunction (EF<40%) often presents with a relatively low-pressure gradient, such as a mean gradient of 30 to 40 mm Hg or less
#31 In LFLG AS, the aortic valve area (AVA) is small, but the pressure gradient across the valve (a measure of stenosis severity) is low due to reduced blood flow. DSE helps determine if the low gradient is due to a truly severe valve narrowing (true severe AS) or if it's a consequence of reduced flow from a less severe obstruction
#32 it is not a replacement for exercise stress testing Dobutamine stress echocardiography (DSE) can be limited in assessing mitral stenosis (MS) due to its potential to alter loading conditions and mask the true severity of the stenosis it can only be used when excercise test no feasible
#34 Dobutamine stress echocardiography (DSE) should not be used instead of exercise to assess the dynamic behaviour of MR because the effect of dobutamine on loading conditions is confounding so it is used only in those who cannot perform a physical exercise test
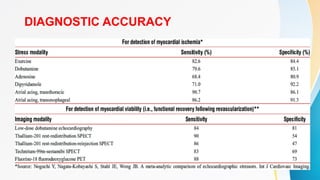
#37 IN VARIOUS METAANALYSIS
stress ecg have sensitivity 63-68 % and specificity 74-77 %
In `DSE average sensitivity for single vessel is 74 % , double vessel is 86% and triple vessel is 92 %
The sensitivity is higher for detection of stenosis in left anterior descending (72%) and RCA (76%) as compared to LCX (55 %)

![In asymptomatic patients with severe MS (mean gradient >10
mm Hg and mitral valve area [MVA] <1.5 cm2
) or
Symptomaticpatients with moderate MS (mean gradient of 5
to 10 mm Hg andMVA > 1.5 cm2
)](https://image.slidesharecdn.com/pharmacologicalstresstesting-250828153255-42f41763/85/PHARMACOLOGICAL-STRESS-TESTING-pptxfgfggf-33-320.jpg)






















![Stresstesting housestaffdidactic_10092014[1]](https://cdn.slidesharecdn.com/ss_thumbnails/stress20testinghousestaff20didactic100920141-141013101956-conversion-gate02-thumbnail.jpg?width=640&height=640&fit=bounds)
![Stress%20 testing housestaff%20didactic_10092014[1]](https://cdn.slidesharecdn.com/ss_thumbnails/stress20testinghousestaff20didactic100920141-141013101524-conversion-gate02-thumbnail.jpg?width=640&height=640&fit=bounds)

























