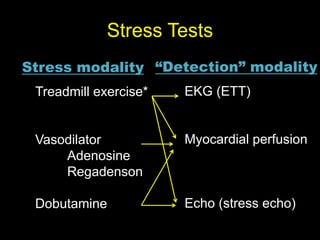
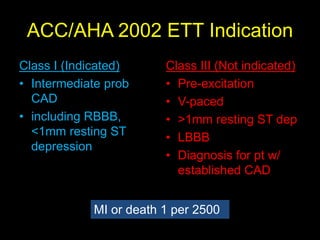
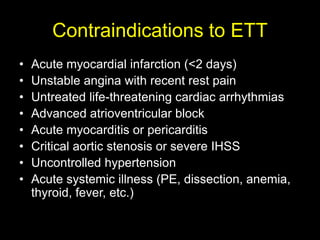
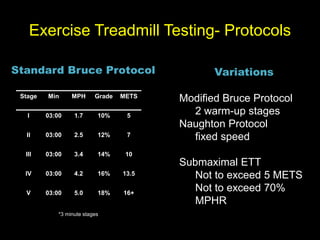
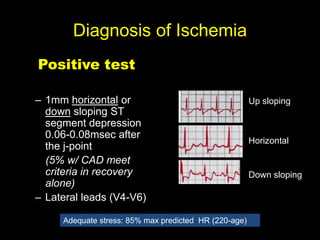
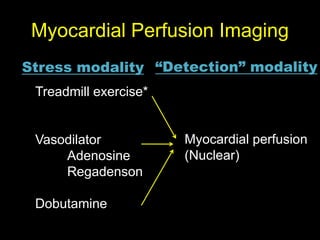
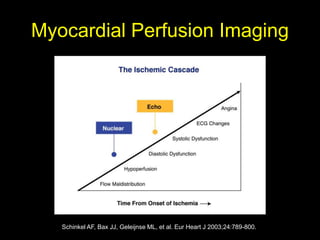
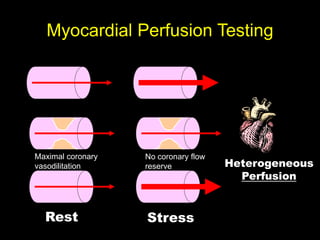
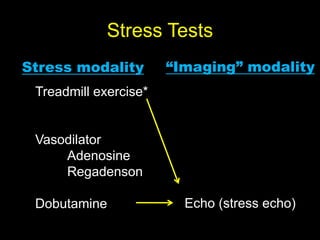
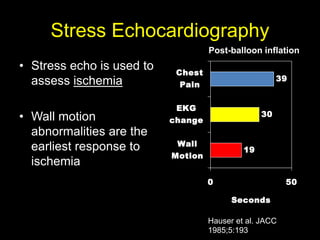
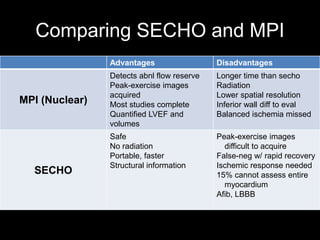
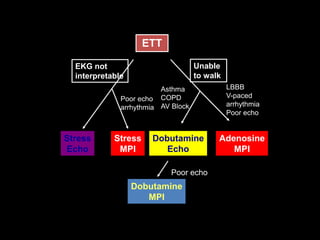
Stress tests use physical or pharmacological stress to detect coronary artery disease. Exercise treadmill testing is commonly used but has limitations. Myocardial perfusion imaging and stress echocardiography can detect ischemia through changes in blood flow or wall motion abnormalities. The appropriate stress test depends on the patient's symptoms, physical limitations, and comorbidities to maximize diagnostic accuracy while avoiding risks.