Downloaded 89 times
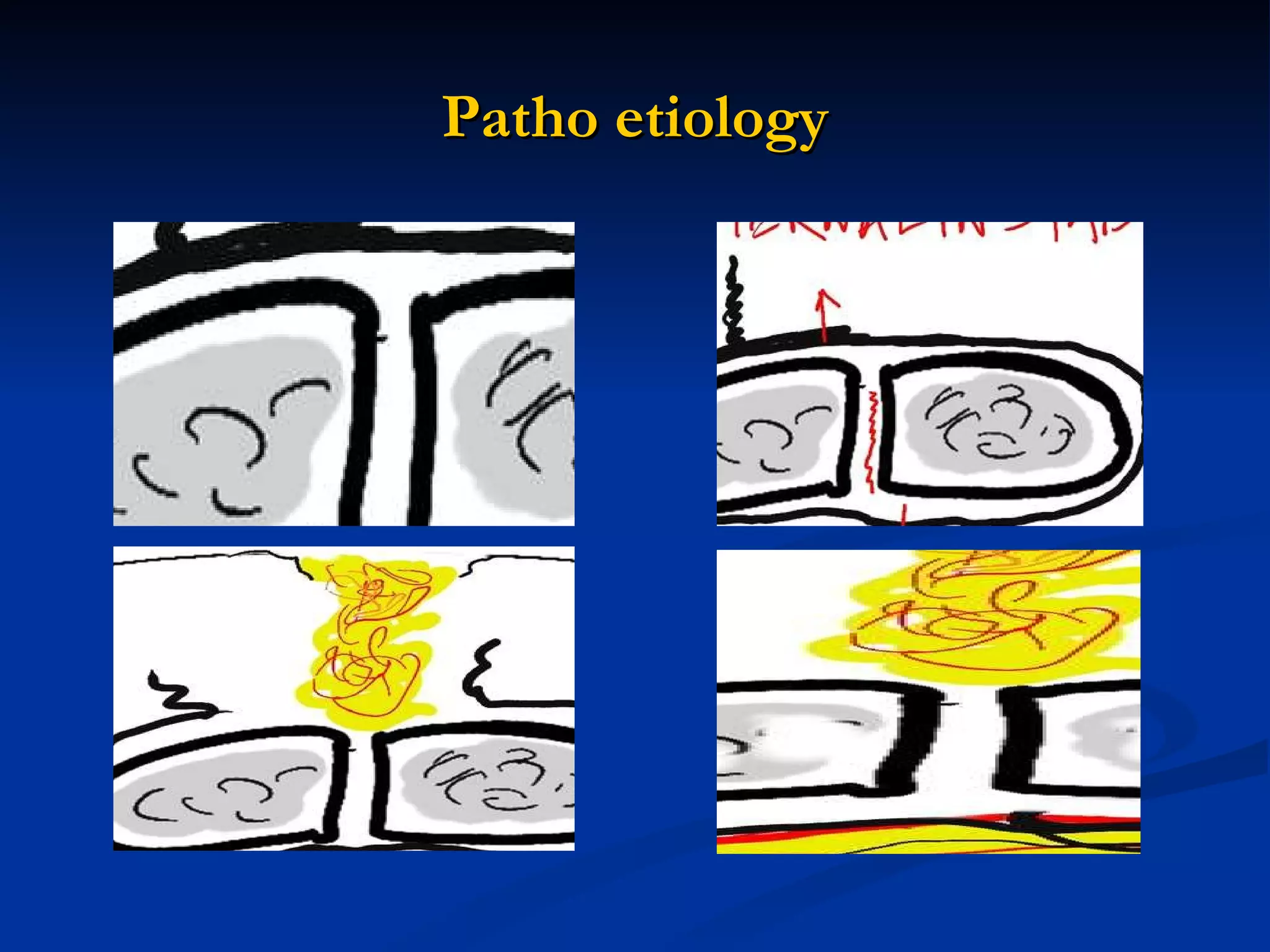

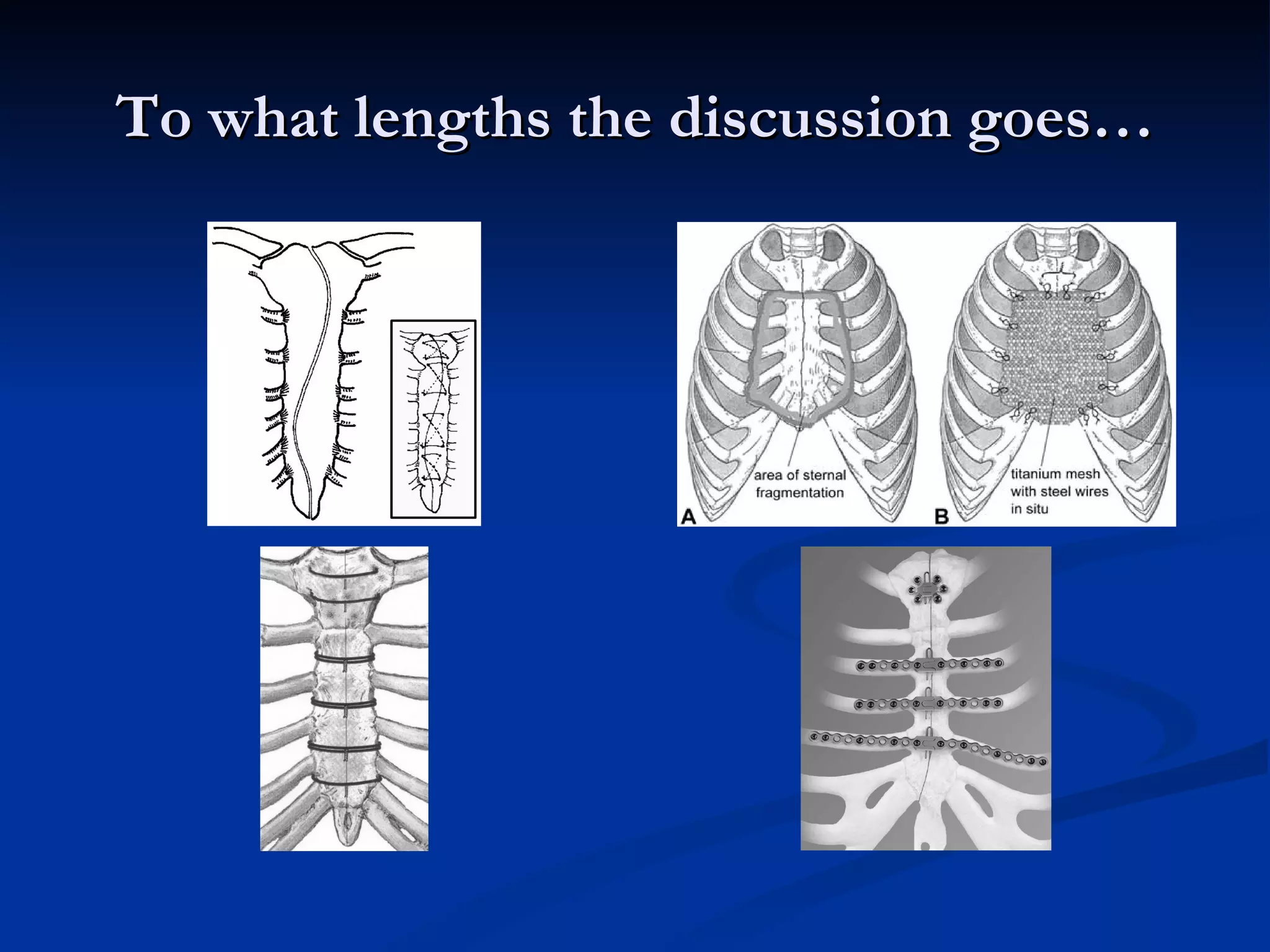
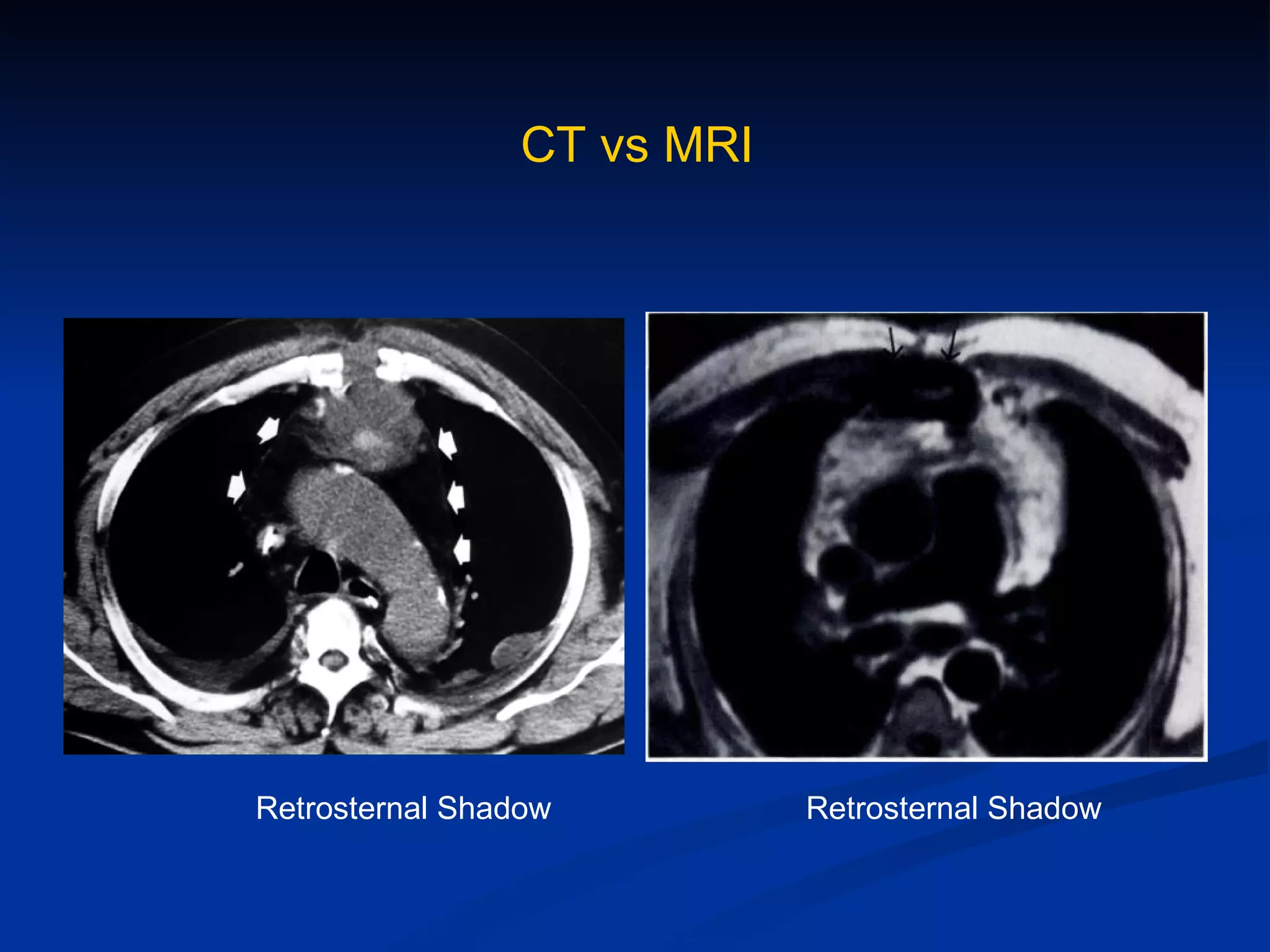
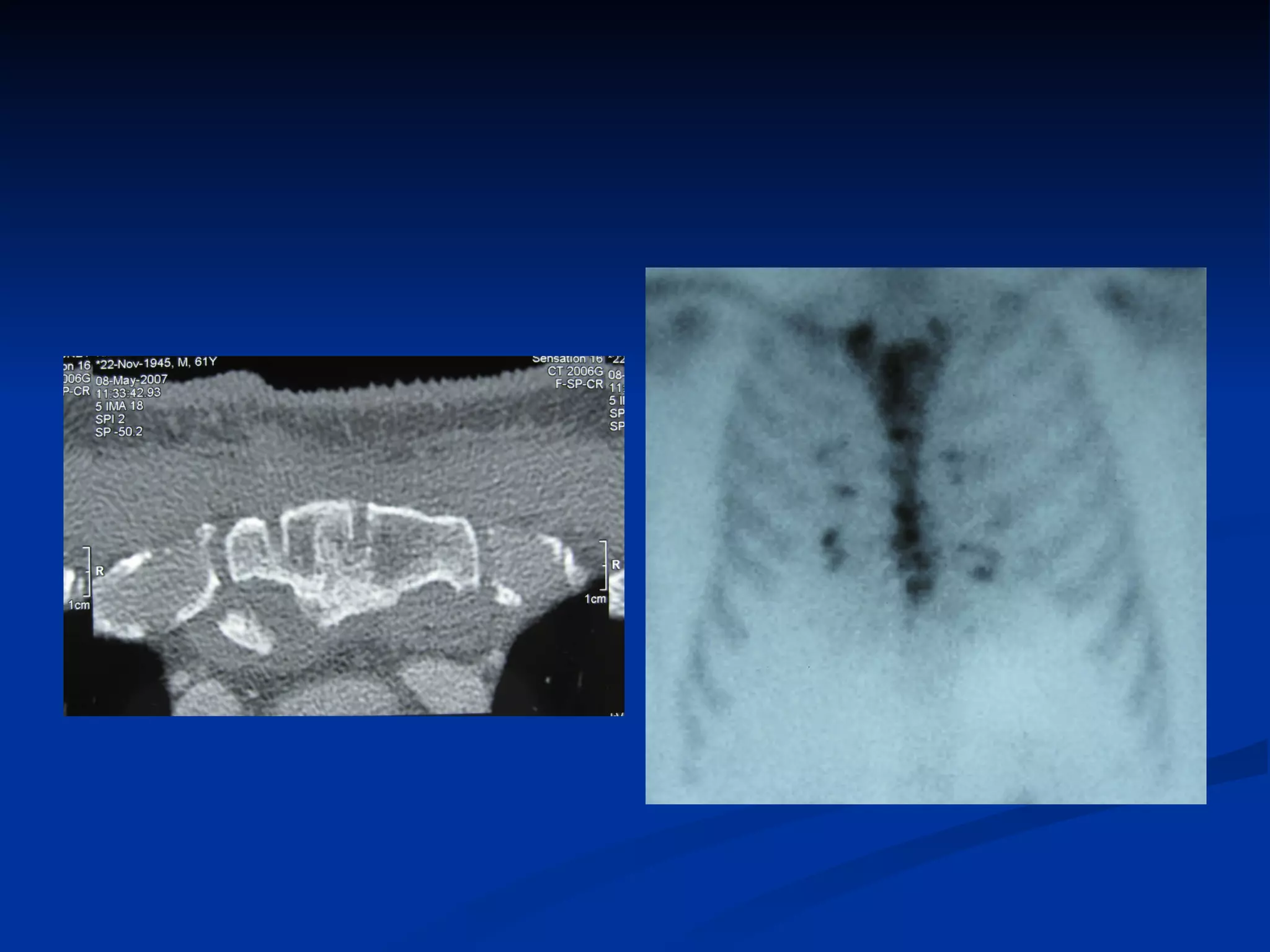
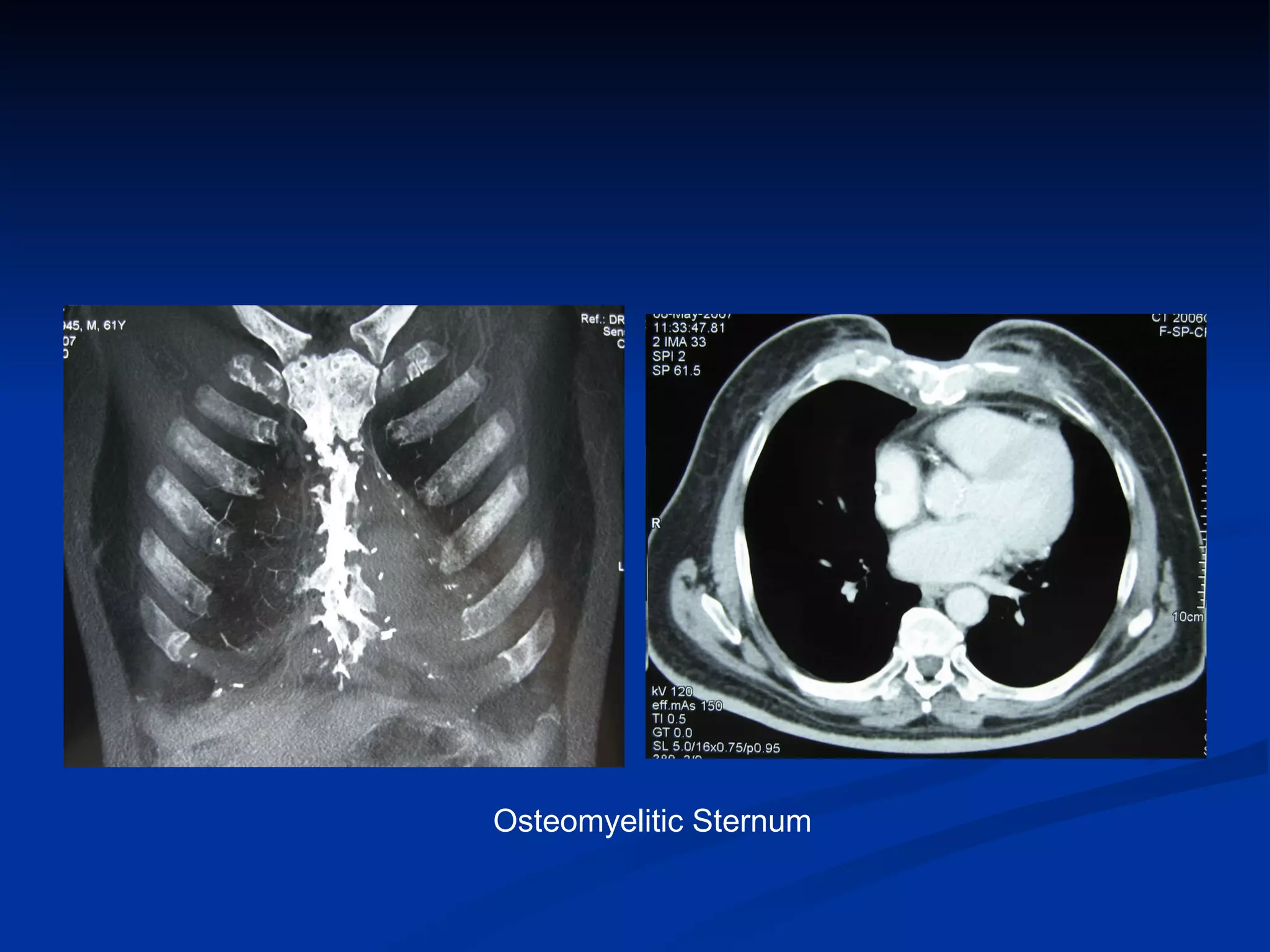
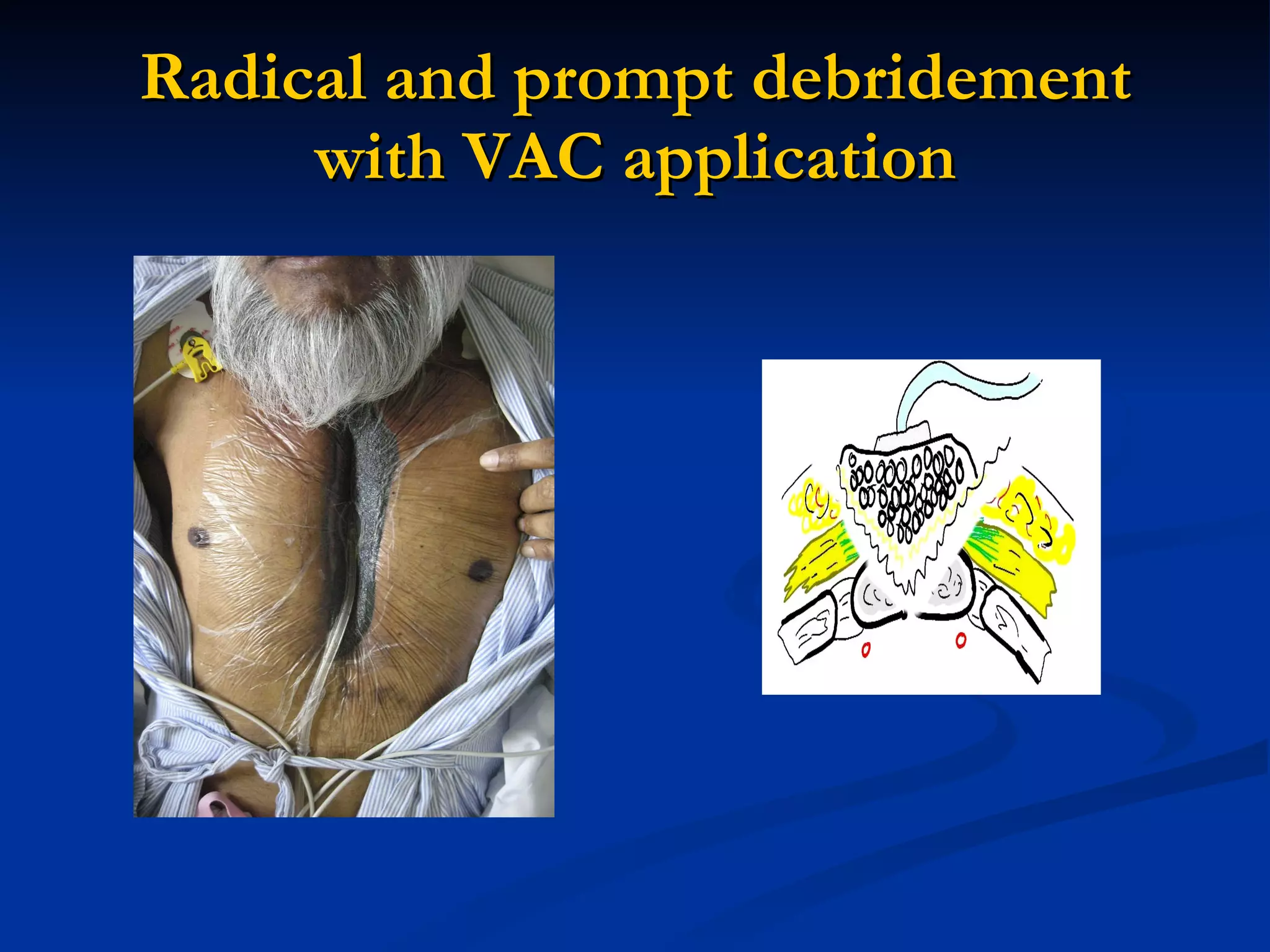



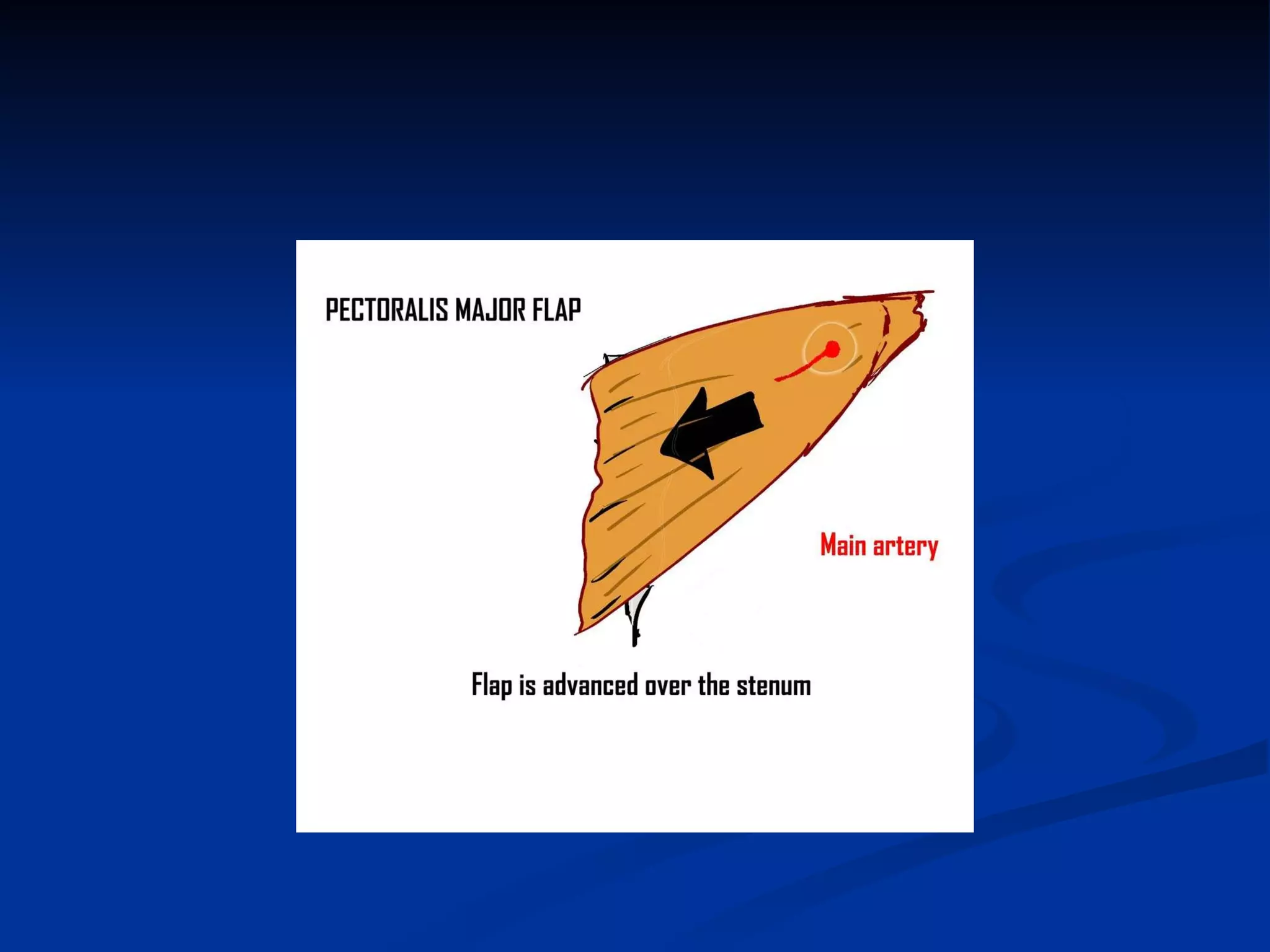
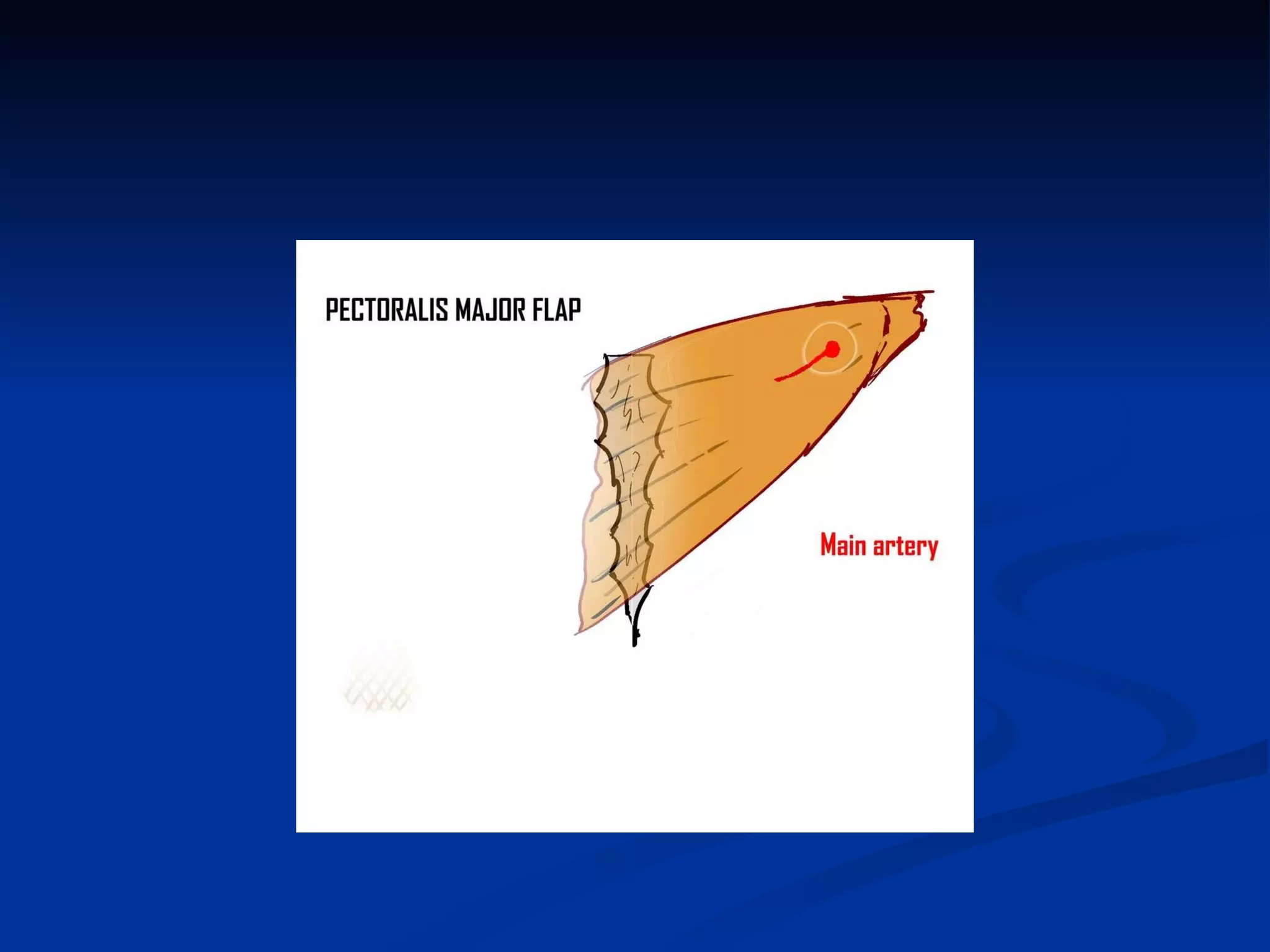
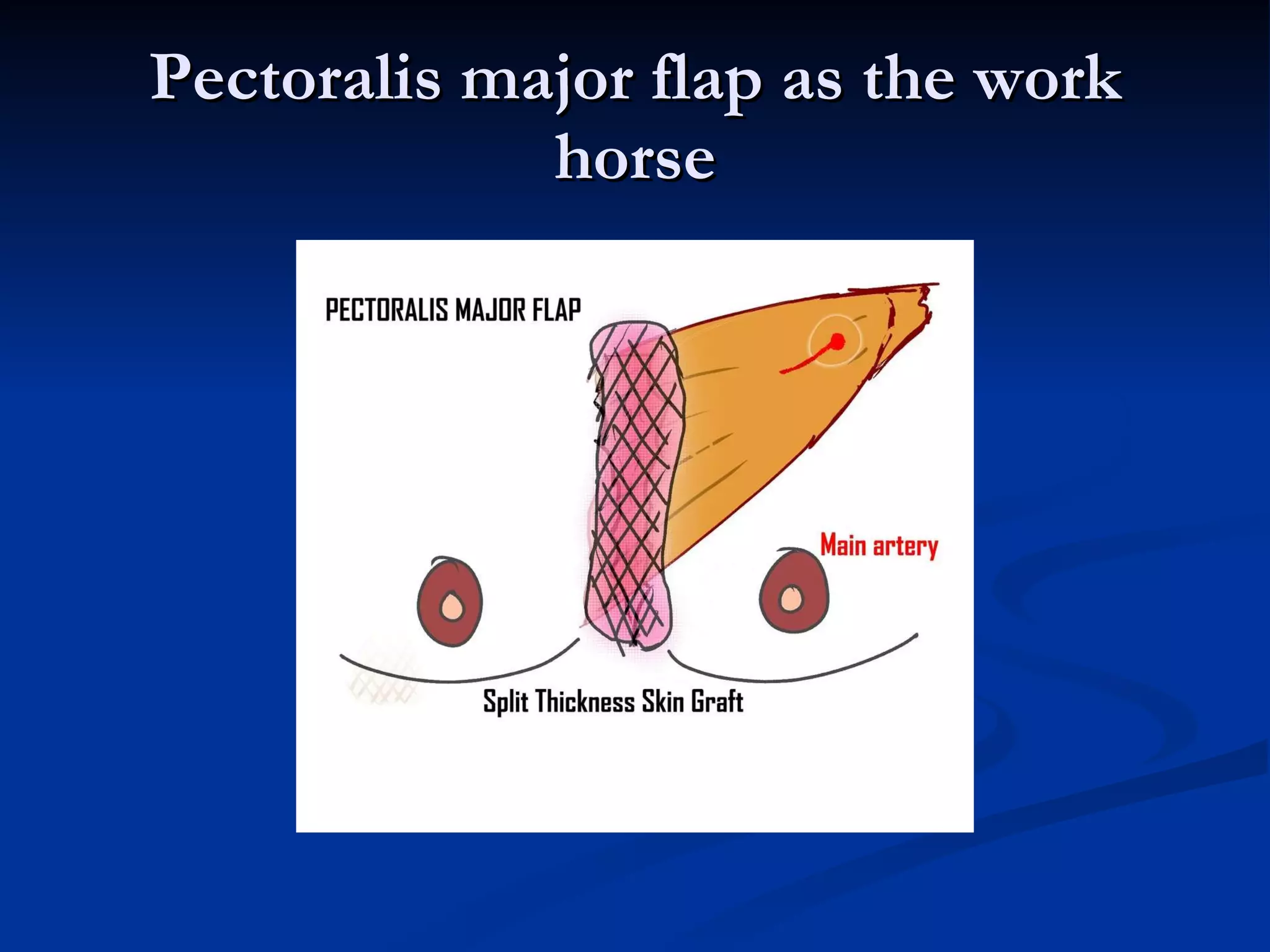







The document discusses median sternotomy and preventing/managing complications. It notes that complications include superficial and deep infection, osteomyelitis, and dehiscence. Risk factors include patient comorbidities, smoking, diabetes, and technical factors like stability. Management involves early recognition, debridement, vacuum-assisted closure, tissue coverage with flaps, and grafting if needed.

































































