1. Video-assisted thoracoscopic surgery (VATS) is a minimally invasive procedure used to diagnose and treat illnesses of the lungs and chest cavity.
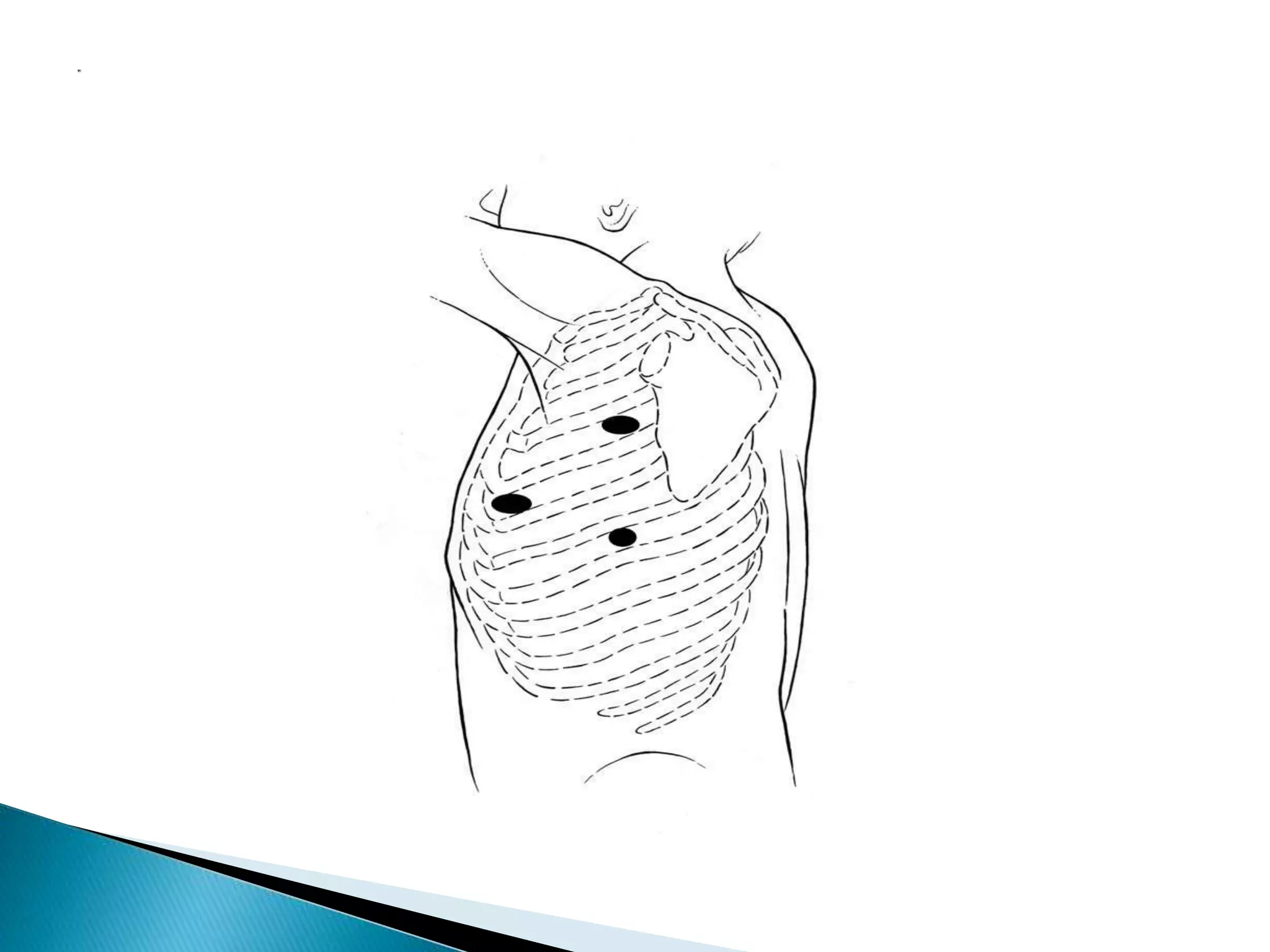
2. VATS involves making small incisions and inserting surgical instruments and a camera to allow the surgeon to see inside the chest. This avoids the need for large incisions.
3. VATS is used for procedures like lung biopsies, removal of parts of the lung, treatment of collapsed lungs, and draining fluid from the chest cavity. It offers benefits like less pain, shorter recovery time, and smaller scars compared to traditional open chest surgery.