The First Attemptto Treat Cancer with X Rays by Doctor Chicotot
16th
OCT 2025/ HISTORY
CHAT GPT
• This is a famous historical illustration titled “The First
Attempt to Treat Cancer with X-Rays by Doctor Chicotot”
(1896).
Context
• Shortly after Wilhelm Conrad Röntgen discovered X-rays in
1895, physicians across Europe began experimenting with
them for medical use.
• Dr. Victor Chicotot, a French physician, was one of the
earliest to apply X-rays in the treatment of cancer.
• The image depicts Chicotot irradiating a patient’s face tumor
with an early X-ray tube.
Importance
• This is one of the earliest recorded attempts at radiation
therapy.
• At the time, the biological effects of radiation (both
therapeutic and harmful) were poorly understood. Many
early pioneers developed severe radiation burns themselves.
• This experiment laid the groundwork for what later evolved
into radiation oncology as a medical specialty.
Artistic/Scientific Value
• The image is often reproduced in textbooks and museums
because it captures the dramatic transition from discovery to
clinical application.
• It symbolizes both the hope of new treatment and the risk of
using technology before its dangers were fully understood.
5.
VARIOUS ARTEFACTS INCT SCAN
17th
OCT 2025/ RADIOLOGY
CHAT GPT
MOTION ARTEFACT METAL/STREAK ARTEFACT RING ARTEFACT
WINDMILL ARTEFACT
DETECTOR ISSUE
Beam hardening from
the dense petrous
OUTFIELD ARTEFACT
PART OUTSIDE THE SFOV
GORHAM-STOUT DISEASE/SYNDROME
19th
OCT 2025/BENIGN
AMIT ROY/Advances in Radiation Oncology (2022)
Aspect Details
Definition
Rare idiopathic disorder with progressive osteolysis (vanishing bone disease) due to vascular/lymphatic
proliferation
Pathology Replacement of bone marrow with angiomatous/lymphangiomatous tissue → bone resorption → fibrous
tissue replacement
Sites Involved Shoulder, pelvis, skull, mandible, ribs, spine
Clinical Features Pain, deformity, pathological fractures, chylothorax if thoracic bones involved
Radiation Therapy Indicated for progressive/symptomatic disease or chylothorax control
Dose Range 36–45 Gy in 1.8–2 Gy fractions (30–45 Gy used; <20 Gy ineffective)
Outcomes 75–80% local control; pain relief; halts further osteolysis
Other Treatments Surgery, bisphosphonates, interferon-α, sirolimus, propranolol
8.
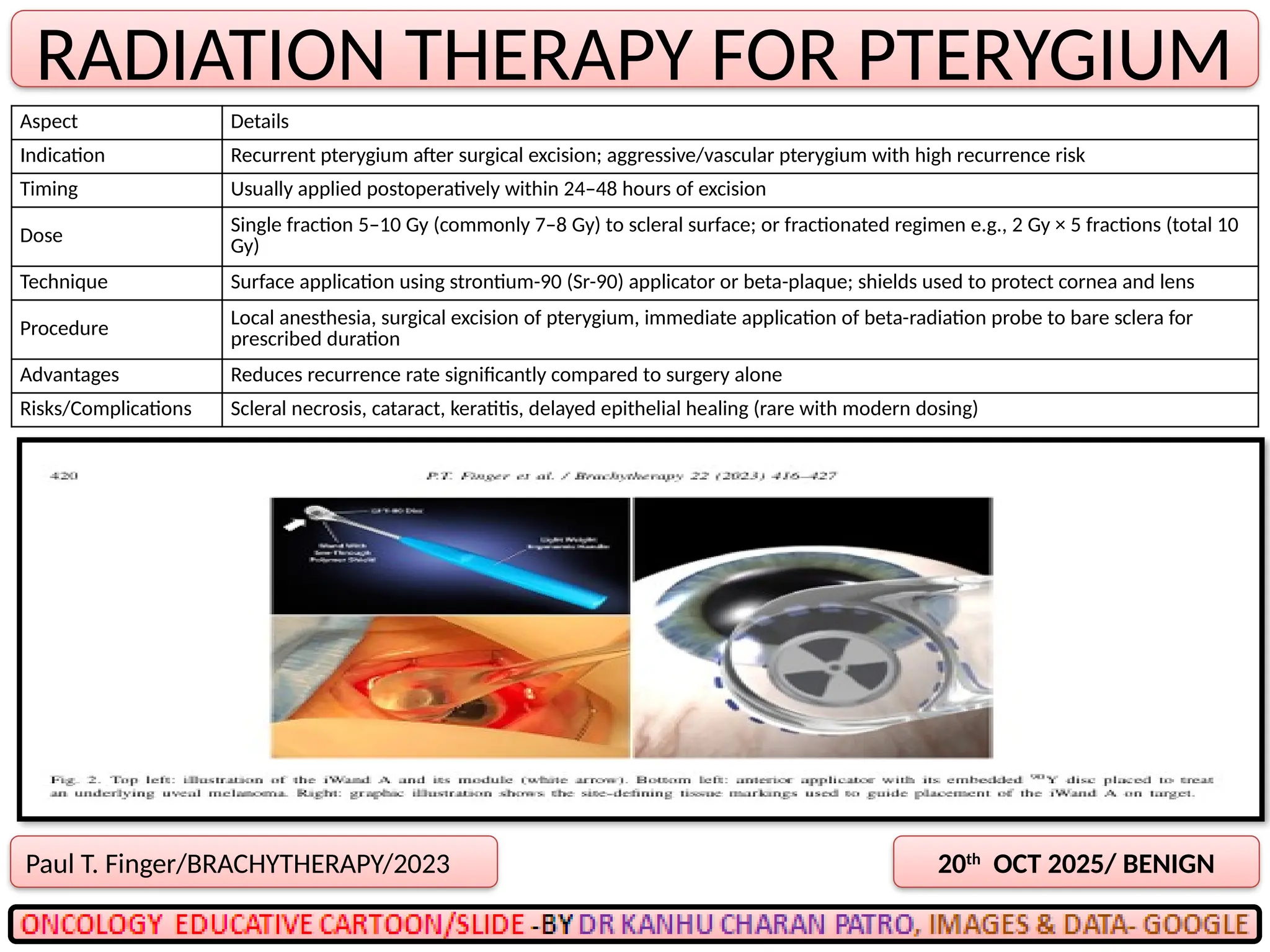
RADIATION THERAPY FORPTERYGIUM
20th
OCT 2025/ BENIGN
Paul T. Finger/BRACHYTHERAPY/2023
Aspect Details
Indication Recurrent pterygium after surgical excision; aggressive/vascular pterygium with high recurrence risk
Timing Usually applied postoperatively within 24–48 hours of excision
Dose
Single fraction 5–10 Gy (commonly 7–8 Gy) to scleral surface; or fractionated regimen e.g., 2 Gy × 5 fractions (total 10
Gy)
Technique Surface application using strontium-90 (Sr-90) applicator or beta-plaque; shields used to protect cornea and lens
Procedure
Local anesthesia, surgical excision of pterygium, immediate application of beta-radiation probe to bare sclera for
prescribed duration
Advantages Reduces recurrence rate significantly compared to surgery alone
Risks/Complications Scleral necrosis, cataract, keratitis, delayed epithelial healing (rare with modern dosing)
9.
RADIATION THERAPY FORORBITAL PSEUDOTUMOR
21st
OCT 2025/ BENIGN
Bruno Fionda/OCULAR IMMUNOLOGY AND INFLAMMATION/2023
Aspect Details
Indication
Refractory orbital pseudotumor (idiopathic orbital inflammation) not responding to corticosteroids or
immunosuppressants. Pain, proptosis, vision-threatening inflammation.
Dose Conventional: 20 Gy in 10 fractions (2 Gy/fraction).Alternative: 20–30 Gy in 10–15 fractions.Low-dose
regimens: 4–10 Gy in 2–5 fractions for palliation/recurrence.
Procedure
External beam radiotherapy (EBRT), typically with 6 MV photons. Immobilization with thermoplastic
mask. CT-based planning, conformal fields/IMRT preferred to spare lens and optic nerve. Field: orbit
only, margin to cover inflammation.
Response
Symptom relief in 60–80% of cases (pain, edema, proptosis).Best results in lymphoid-predominant
histology; fibrotic type responds less.
Toxicity Usually minimal with low doses. Possible late effects: cataract, dry eye, retinopathy (rare at ≤20 Gy).
10.
SWI IMAGE INDIFFERENTIATING ACOUSTIC SCHWANNOMA AND MENINGIOMA
22nd
OCT 2025/BRAIN
MINKOOK SEO/ (KSMRM)/2020
11.
SWI IMAGE INDIFFERENTIATING LOW GRADE AND HIGH GRADE GLIOMA
23rd
OCT 2025/BRAIN
Omer Aydin / Pol J Radiol, /2017
12.
DYNAMIC CONTRAST IMAGEAND DIFFERENCE FROM CONTRAST IMAGE
24th
OCT 2025/BRAIN
Omer Aydin / Pol J Radiol, /2017
Feature Contrast MRI DCE-MRI
Type Static Dynamic
DESCRIPTION
A standard MRI scan with a
contrast agent (typically
Gadolinium) to highlight blood
vessels, tissues, or lesions at a
specific time point.
A functional imaging technique where
multiple images are taken over time
after contrast injection to study the
dynamics of contrast uptake and
washout in tissues
Purpose Better tissue contrast Evaluate tissue
vascularity/permeability
Image Acquisition One or few time points Repeated sequences over time
Data Type Anatomical, qualitative Functional, quantitative/kinetic
Analysis Visual inspection
Pharmacokinetic modeling (e.g.,
Ktrans, Ve, Kep)
Parameters Anatomical only Functional (Ktrans, Ve, etc.)
Common Use Tumor detection Tumor grading, treatment response
13.
K-TRANS IN DCEIMAGES WITH RESPET TO GLIOMA
25th
OCT 2025/BRAIN
Omer Aydin / Pol J Radiol, /2017
1. K-trans (Volume Transfer Constant)
2. A quantitative parameter from DCE MRI.
3. Reflects how quickly contrast agent moves from blood plasma into the extracellular extravascular space (EES).
4. High K-trans = high vascular permeability and often increased blood flow
5. K^trans (Volume Transfer Constant) is a key pharmacokinetic parameter derived from Dynamic Contrast-Enhanced
MRI (DCE-MRI).
6. It reflects vascular permeability and perfusion, specifically the rate at which contrast agent moves from the blood
plasma into the extravascular extracellular space (EES).
7. In gliomas, K^trans values vary depending on tumor grade due to differences in angiogenesis, blood-brain barrier
(BBB) integrity, and vascular permeability.
Glioma Type / Grade K^trans Value Interpretation Clinical Significance
Low-Grade Glioma (Grade II) • Low (near-
normal)
Intact BBB, low vascular
permeability
Minimal or no enhancement on DCE; low
K^trans helps differentiate from high-grade
tumors
Anaplastic Glioma (Grade III) • intermediate
Partially disrupted BBB,
increased but variable
permeability
Moderate enhancement and heterogeneous
K^trans; may aid in treatment planning and
progression monitoring
Glioblastoma Multiforme
(Grade IV) • High
Severely disrupted BBB, high
angiogenesis and
permeability
High K^trans in enhancing regions;
correlates with aggressiveness and poor
prognosis
Pseudoprogression / Radiation
Necrosis Variable (often high)
Leaky vessels post-
treatment; not due to tumor
May mimic recurrence; advanced imaging +
clinical correlation needed
14.
Borrmann’s Types ofAdvanced Gastric Cancer
26th
OCT 2025/STOMACH
Cristina Díaz del Arco/cancers/2021
15.
FAPI PET =Fibroblast Activation Protein Inhibitor PET
27th
OCT 2025/PET
Yuriko Mori/RSNA/2023
1. FDG PET has limitations in tumors with low glycolytic activity (e.g., mucinous tumors, some hepatocellular cancers).
2. Tumor stroma can be a more universal target—present even when tumor cells have low metabolic rate.
3. FAPI PET shows very high tumor-to-background ratio due to minimal physiological uptake in most normal tissues.
4. Can be performed without fasting and often within 10–20 minutes post-injection (faster workflow).
5. cancers with low FDG uptake:
1. Prostate cancer (especially PSMA-negative)
2. Hepatocellular carcinoma (HCC)
3. Mucinous adenocarcinomas (colon, ovary, pancreas)
4. Sarcomas
6. Head & neck cancers (for high-contrast tumor delineation)
7. Peritoneal carcinomatosis (better detection vs FDG)
8. Tumor staging, restaging, and radiotherapy planning (better GTV delineation
Feature FDG PET FAPI PET
Target Glucose metabolism (GLUT transporters, hexokinase) Fibroblast Activation Protein (tumor stroma)
Physiological uptake High in brain, heart, bowel, urinary tract Low in most normal tissues (except healing wounds,
inflammation, uterus, pancreas)
Preparation Fasting, control of blood glucose No fasting, minimal prep
Scan timing 60 min post-injection 10–20 min post-injection
Best for Highly glycolytic tumors (lung, lymphoma, melanoma) Low-FDG tumors, tumor delineation, fibrosis imaging
Limitations Low uptake in some tumors, high background in
brain/heart
Still investigational, false positives in inflammation &
healing
Regulatory status Widely approved Mostly research / early clinical use
16.
FAPI PET =Fibroblast Activation Protein Inhibitor PET
28th
OCT 2025/PET
Yuriko Mori/RSNA/2023
17.
Role of FAPIPET in Gastric Cancer
29th
OCT 2025/STOMACH
Yuyun sun/RSNA/2024
68Ga-FAPI PET/CT had higher accuracy in diagnosis of gastric mucinous adenocarcinoma or signet ring cell carcinoma compared
with 18
F-FDG PET/CT and demonstrated the potential to improve treatment strategies and predict prognosis.
18.
CRAB AND SLIMCRAB IN MYELOMA
30th
OCT 2025/STOMACH
PINTREST
19.
SPLENIC CONSTRAINTS INABDOMINAL RT
31st
OCT 2025/OAR
K KESWANI/CLINICAL ONCOLOGY/2022
SILVIA BISELLO/CURRENT ONCOLOGY/2022
20.
MRI PICTURES OFVASCULAR ANOMALIES
1st
NOV 2025/BRAIN
GOOGLE
DURAL AVF
NO NIDUS
CAVERNOMA
POPCORN
DEVELOPMENTAL
VENOUS ANAOMOLY
CAPUT MEDUSAE
SIGN
AVM- NIDUS
BAG OF WORM
CAPILLARY
TALANGECTESIA
SACCULAR
ANEURYSM
(InPACT) Trial penis– Target Volume for Neoadjuvant
4th
NOV 2025/PENIS
Sian Cooper/IJROBP/2025
24.
(InPACT) Trial penis- Target Volume for post pelvic Sx
5th
NOV 2025/PENIS
Sian Cooper/IJROBP/2025
25.
(InPACT) Trial penis- Target Volume for No pelvic Sx
6th
NOV 2025/PENIS
Sian Cooper/IJROBP/2025
26.
WHY SHOULD WEINCLUDE PREPUBIC FAT IN THE TARGET?
7th
NOV 2025/PENIS
Sian Cooper/IJROBP/2025
27.
(InPACT) Trial penis- Target Volume for pubic fat
8th
NOV 2025/PENIS
Sian Cooper/IJROBP/2025
A
V
O
I
D
28.
(InPACT) Trial penis– OAR DOSE CONSTRAINTS
9th
NOV 2025/PENIS
Sian Cooper/IJROBP/2025
29.
(InPACT) Trial penis– Neoadjuvant DOSE SCHEDULE
10th
NOV 2025/PENIS
Sian Cooper/IJROBP/2025
Region / Situation Indication Dose (25 #)
Macroscopic pelvic nodes
(CTV_P) Gross pelvic nodal disease 45 Gy
Macroscopic inguinal nodes
(CTV_I) Gross inguinal nodal disease 45 Gy
Pelvic/inguinal nodes If inguinal disease present or
staging unknown 45 Gy
Prepubic fat All patients 45 Gy
Common iliac nodes Only if pelvic nodal
involvement
45 Gy
30.
Region / SituationIndication Dose (25 fractions)
Macroscopic pelvic nodes
(CTV_P)
Boost 54 Gy
Macroscopic inguinal nodes
(CTV_I)
Boost 57 Gy
Pelvic nodes High-risk inguinal disease (≥2
nodes, extracapsular spread)
54 Gy
Inguinal nodes
High-risk (≥2 nodes,
extracapsular spread)
54 Gy (boost to 57 Gy if gross
disease)
Inguinal nodes
Low-risk (1 node, no
extracapsular spread) 45 Gy
Prepubic fat All patients 54 Gy (boost if gross disease)
Common iliac If pelvic nodal disease 45 Gy (boost to 57 Gy if gross
disease)
(InPACT) Trial penis - POST OP DOSE SCHEDULE- No Pelvic Sx
11th
NOV 2025/PENIS
Sian Cooper/IJROBP/2025
31.
(InPACT) Trial penis- POST OP DOSE SCHEDULE- Pelvic Sx
12th
NOV 2025/PENIS
Sian Cooper/IJROBP/2025
Region / Situation Indication Dose (25 fractions)
Macroscopic pelvic nodes (CTV_P) Boost 54 Gy
Macroscopic inguinal nodes
(CTV_I)
Boost 57 Gy
Pelvic nodes Positive pelvic nodal dissection 54 Gy
Pelvic nodes Negative pelvic nodal dissection No RT
Inguinal nodes
High-risk disease (≥2 nodes,
extracapsular spread, or gross
disease)
54 Gy (boost to 57 Gy if gross)
Inguinal nodes
Low-risk (1 node, no extracapsular
spread) 45 Gy
Prepubic fat All patients 54 Gy
Common iliac If pelvic disease at dissection 54 Gy (boost if gross disease)
32.
(InPACT) Trial penis- POST OP DOSE TRAGET COVERGAE
13th
NOV 2025/PENIS
Sian Cooper/IJROBP/2025
33.
CONSTRAINTS IN ABDOMINALRT- SOLITARY KIDNEY
14th
NOV 2025/OAR
SILVIA BISELLO/CURRENT ONCOLOGY/2022
34.
🎗"Breathe with Care"– Lung Cancer Awareness 🎗
15th
NOV 2025/ PUBLIC
CHAT GPT
Inhale hope, exhale the fear,
Lung cancer signs — let’s keep them clear.
A cough that stays, breath that’s tight,
Check it early, win the fight.
Smoking, smog, and toxic air,
Take a stand — show you care.
This November, spread the word,
Let every breath of life be heard.
Every breath is a battle cry,
For those who fight, and those who die.
Smoke and silence steal the years,
But hope still rises through the tears.
It's not just lungs — it's life at stake,
So raise your voice, be wide awake.
November calls — stand tall, stand true,
The fight for lungs begins with you
![DR KANHU CHARAN PATRO
M.D, D.N.B[RT], MBA, FICRO, FAROI, PDCR, CEPC
www.slideshare.net/search/slideshow?searchfrom=header&q=oncology+cartoons
www.facebook.com/oncologycartoons/photos_albums
116th
Volume/NOVEMBER 2025
ONCOLOGY CRATOONS EDUCATIVE E-BOOK](https://image.slidesharecdn.com/nov2025-251029034719-4f3d9eee/75/NOV-2025-Oncology-Cartoons-By-Dr-Kanhu-Charan-Patro-1-2048.jpg)