INTRODUCTION The causesof acute hypertension in a variety of brain injury paradigms The effects of hypertension on the cerebral vasculature The management of acutely elevated blood pressure in neurologic disease
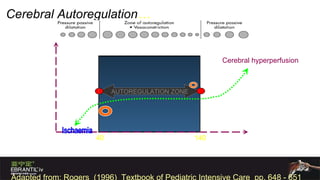
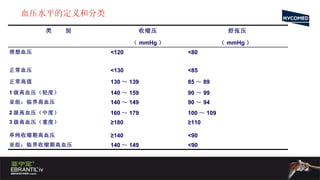
AUTOREGULATION ZONE SystemicBlood Pressure / MAP Cerebral Autoregulation … 40 140 Cerebral hyperperfusion Cerebral Blood Flow Adapted from: Rogers (1996) Textbook of Pediatric Intensive Care pp. 648 - 651
7.
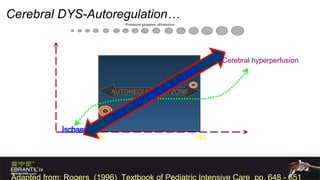
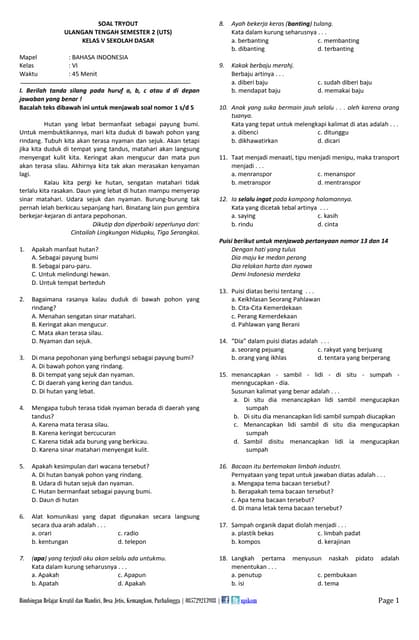
AUTOREGULATION ZONE AUTOREGULATIONZONE Systemic Blood Pressure / MAP Cerebral DYS-Autoregulation… 40 140 Cerebral hyperperfusion Cerebral Blood Flow Adapted from: Rogers (1996) Textbook of Pediatric Intensive Care pp. 648 - 651 DYS - AUTOREGULATION
8.
9.
Hypertension in acutebrain insult Presence of chronic hypertension Suspected IICP Age Etiology of hemorrhage Multiple injury Time since onset Pain ,anxiety, withdrawal medications and certain illicit drugs
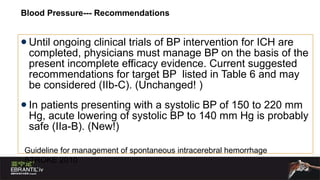
Blood Pressure--- RecommendationsUntil ongoing clinical trials of BP intervention for ICH are completed, physicians must manage BP on the basis of the present incomplete efficacy evidence. Current suggested recommendations for target BP listed in Table 6 and may be considered (IIb-C). (Unchanged! ) In patients presenting with a systolic BP of 150 to 220 mm Hg, acute lowering of systolic BP to 140 mm Hg is probably safe (IIa-B). (New!) Guideline for management of spontaneous intracerebral hemorrhage STROKE 2010
14.
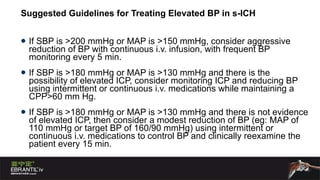
Suggested Guidelines forTreating Elevated BP in s-ICH If SBP is >200 mmHg or MAP is >150 mmHg, consider aggressive reduction of BP with continuous i.v. infusion, with frequent BP monitoring every 5 min. If SBP is >180 mmHg or MAP is >130 mmHg and there is the possibility of elevated ICP, consider monitoring ICP and reducing BP using intermittent or continuous i.v. medications while maintaining a CPP>60 mm Hg. If SBP is >180 mmHg or MAP is >130 mmHg and there is not evidence of elevated ICP, then consider a modest reduction of BP (eg: MAP of 110 mmHg or target BP of 160/90 mmHg) using intermittent or continuous i.v. medications to control BP and clinically reexamine the patient every 15 min.
15.
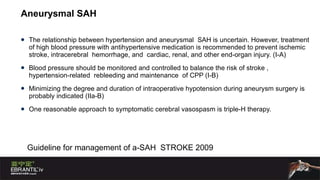
Aneurysmal SAH Therelationship between hypertension and aneurysmal SAH is uncertain. However, treatment of high blood pressure with antihypertensive medication is recommended to prevent ischemic stroke, intracerebral hemorrhage, and cardiac, renal, and other end-organ injury. (I-A) Blood pressure should be monitored and controlled to balance the risk of stroke , hypertension-related rebleeding and maintenance of CPP (I-B) Minimizing the degree and duration of intraoperative hypotension during aneurysm surgery is probably indicated (IIa-B) One reasonable approach to symptomatic cerebral vasospasm is triple-H therapy. Guideline for management of a-SAH STROKE 2009
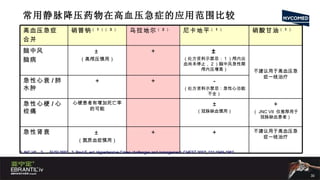
硝酸甘油 (nitroglycerin) 血管扩张剂 作用机制 主要扩张静脉,大剂量扩张动脉 优势 扩张冠脉作用明显 缺点 1. 头痛,心动过速和低血压是首要付作用 2. 颅内压高、青光眼禁用 3. 血容量过低时谨防体位性低血压 4. 个体对剂量敏感性差别大,易耐药 应用范围: JNC VII 仅推荐用于 -- 高血压合并心梗 / 心绞痛 冠脉综合症 由于硝酸甘油对动脉扩张弱, JNC VII 未推荐用于其它高血压急症 JNC VII. Paul E, et al. Hypertensive Crises challenges and management. CHEST 2007; 131:1949-1962 , Andrew R., et al. Current Diagnosis and Management of Hypertensive Emergency. Seminars in Dialysis- Vol 19, No 6 (Nov.-Dec) 2006 pp.502-512
32.
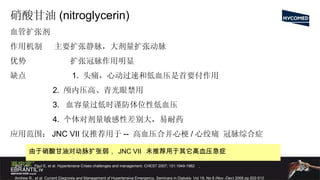
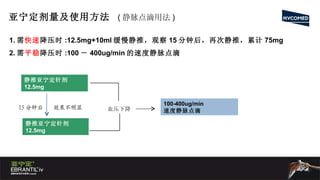
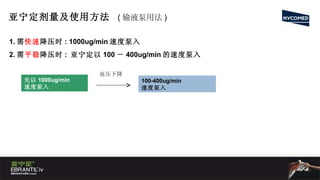
硝普钠 (nitroprusside sodium)血管扩张剂 作用机制:硝普钠中的亚硝基是它的扩血管基团,可分解为 NO 引起血 管扩张。由于 NO 极不稳定,停止滴注 1 ~ 2min 血压即回升 优势 1. 起效很快,作用时间短 2. 降压作用强 3. 降压反应率高 95-100% ( 3 ) 应用范围:大部分高血压患者 1 。 Paul E, et al. Hypertensive Crises challenges and management. CHEST 2007; 131:1949-1962 2 。 William J., et al. Management of Hypertensive Crises. Current Hypertention Reports 2003, 5:486-492 3 。 Michael M. Hirschl. Guidelines for the drug treatment of hypertensive crises. Drugs 50(6): 991-1000,1995
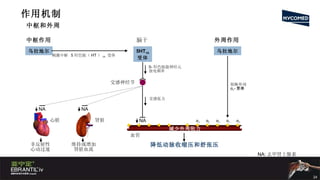
可乐定( CLONIDINE )Alpha 2adrenergic agonist acts on inhibitory neurons in the medullary vasomotor center causing a decrease in sympathetic outflow to the periphery, and resultant vasorelaxalation in both resistance and capacitance
Barbiturates Allosteric activationGABA receptor Peripheral venodilation and pooling of blood due to decreased sympathetic nervous system outflow from CNS.
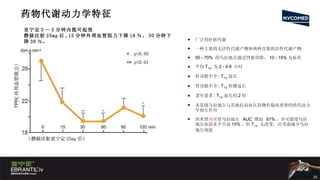
#6 This relationship between ICP, mean arterial pressure (MAP), and cerebral perfusion pressure (CPP) can be appreciated by the equation CPP=MAP-ICP (1). In normal children ICP is <20 mm Hg, and MAP is 70-80 mm Hg, which provides a normal CPP ranging from 50-60 mm Hg (1). Thus, accordingly an increase in ICP, or decrease in MAP can decrease blood flow into the brain. When CPP is <40 mm Hg, ischemia occurs as proper cerebral blood flow (CBF) cannot be maintained (1). This simplified equation attempts to explain a very complicated pathophysiologic process. Controlled by chemical mediators that produce vasoconstriction and vasodilatation of the blood vessels, CBF is constantly changing to meet the brain's metabolic demands. The most potent chemical mediator is the arterial partial pressure of carbon dioxide (pCO2), which is directly proportional to CBF. The arterial partial pressure of oxygen (pO2) is indirectly proportional to CBF, but it is not as potent a vasoactive mediator as pCO2. In the acute management of the patient with a severe head injury, these values are manipulated via intubation and mechanical ventilation to maximize CPP.