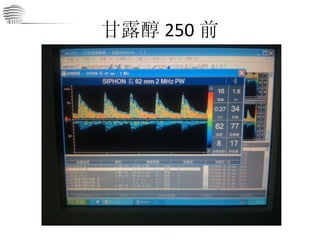
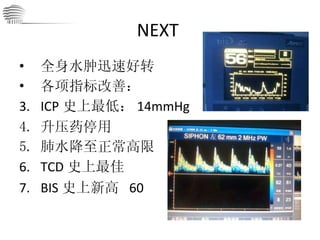
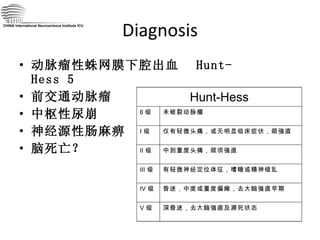
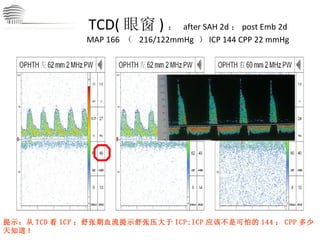
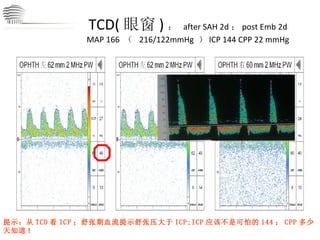
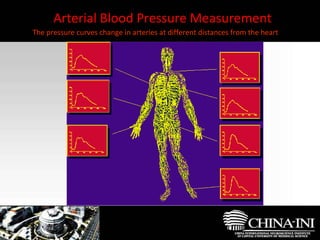
TCD( 眼窗 ): after SAH 2d ; post Emb 2d MAP 166 ( 216/122mmHg ) ICP 144 CPP 22 mmHg 提示:从 TCD 看 ICP ;舒张期血流提示舒张压大于 ICP;ICP 应该不是可怕的 144 ; CPP 多少天知道 ! CHINA International Neuroscience Institute ICU
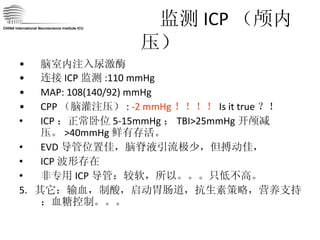
21.
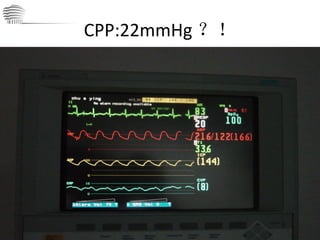
BRAIN DEATH ?NO! At Least Not Yet! CBF 存在;当然不是足够 虽然 CPP 只有 22 mmHg :数字游戏? 脑死亡诊断不成立 ,至少暂时不成立。 状态: ICP ↑ ↑ CPP ↓ ↓ CBF ↓ ↓ 针对改善 CBF 我们还能做什么? CHINA International Neuroscience Institute ICU
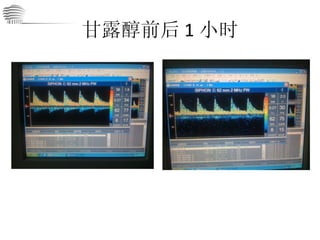
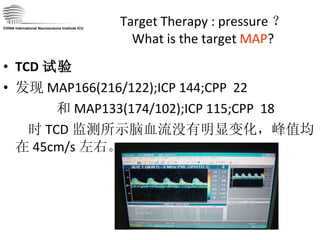
Target Therapy :pressure ? What is the target MAP ? TCD 试验 发现 MAP166(216/122);ICP 144;CPP 22 和 MAP133(174/102);ICP 115;CPP 18 时 TCD 监测所示脑血流没有明显变化,峰值均在 45cm/s 左右。 CHINA International Neuroscience Institute ICU
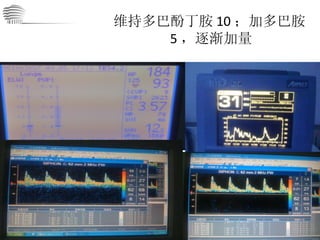
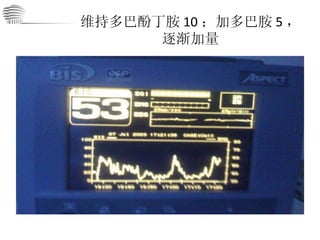
D3 从压力到容量改变血流动力学状态 提高 CO 减少垂体后叶素:减少外周血管收缩,降低后负荷。 加用多巴酚丁胺 8 μ g/kgmin : 增加心排,减低后负荷 扩容:万汶,白蛋白,血浆;保障基本前负荷 监测血流动力学变化; CO 和 CBF ( TCD ); 试验结果:期待 ing 。。。 CHINA International Neuroscience Institute ICU
39.
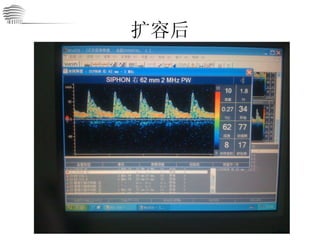
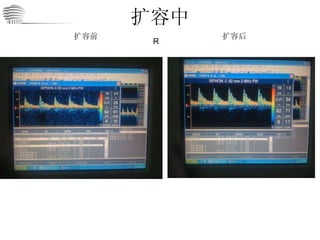
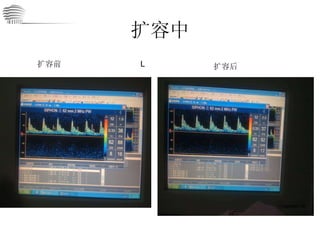
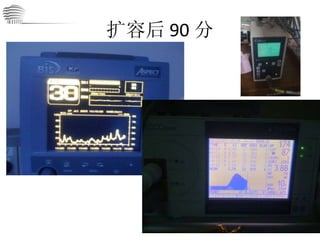
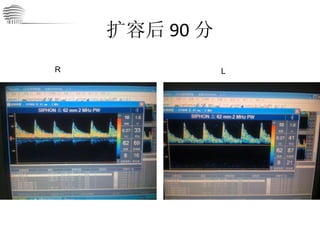
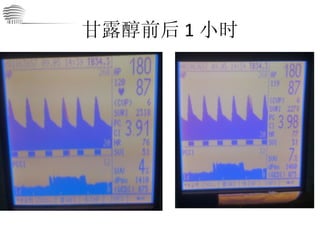
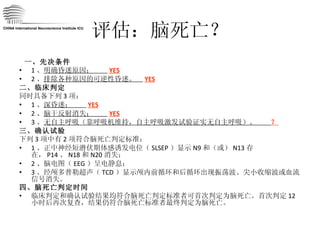
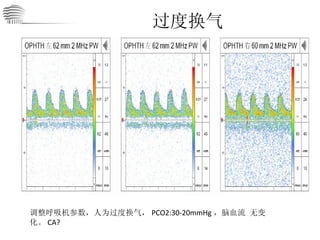
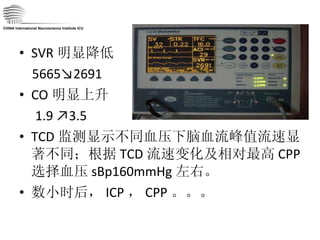
SVR 明显降低 5665↘2691CO 明显上升 1.9 ↗3.5 TCD 监测显示不同血压下脑血流峰值流速显著不同;根据 TCD 流速变化及相对最高 CPP 选择血压 sBp160mmHg 左右。 数小时后, ICP , CPP 。。。 CHINA International Neuroscience Institute ICU
40.
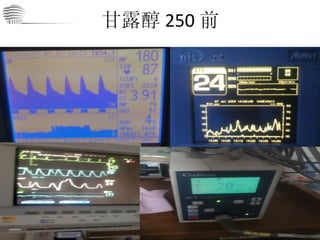
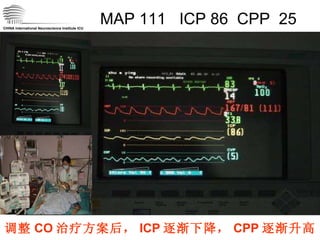
MAP 111 ICP 86 CPP 25 CHINA International Neuroscience Institute ICU 调整 CO 治疗方案后, ICP 逐渐下降, CPP 逐渐升高
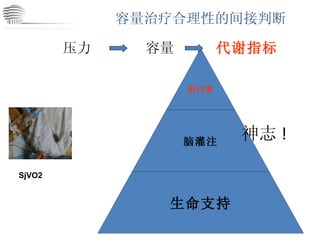
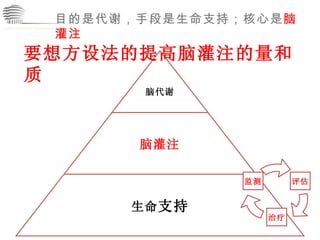
PART 1 小结 CHINA International Neuroscience Institute ICU 不要忘记了我们最初的目的: 不是压力 是 灌注 !
43.
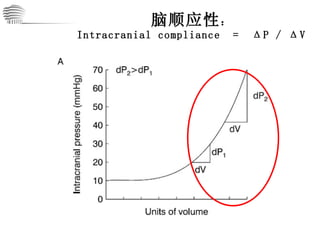
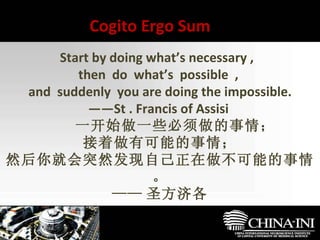
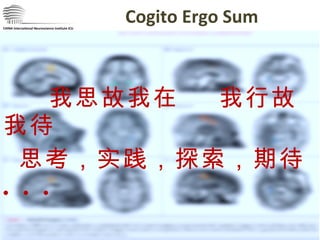
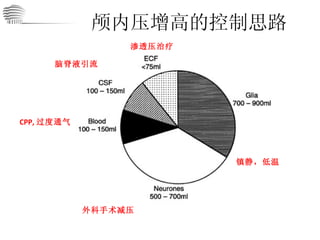
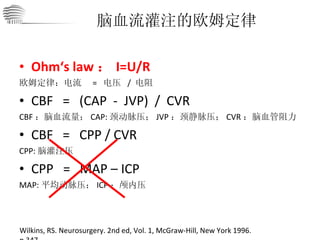
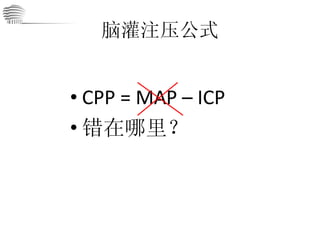
颅内压 ICP颅腔内容物:神经元,神经胶质细胞,血液,脑脊液,细胞外液 (病理情况下:如内生骨瘤,转移瘤,空气,异物。。。) [1] 任何一项容积发生变化和 / 或出现新的占位(如血肿)等都会使 ICP 发生变化,首发因素的程度和速度等决定了 ICP 变化的程度 [2] 脑顺应性: Intracranial compliance = Δ P / Δ V 1. Head Injury . Peter Reilly and Ross Bullock. Chapman & Hall, London. 1997; 19. Management of Intracranial Pressure And Cerebral Perfusion. 386 2. John M. Turner. Textbook of neuroanaesthesia and intensive care.52-64 , Greenwich Medical Media LTD, 2000. 经典的颅内压力容积曲线( Monro-Kellie 假说)
颅内压 ICP颅腔内容物:神经元,神经胶质细胞,血液,脑脊液,细胞外液 (病理情况下:如内生骨瘤,转移瘤,空气,异物。。。) [1] 任何一项容积发生变化和 / 或出现新的占位(如血肿)等都会使 ICP 发生变化,首发因素的程度和速度等决定了 ICP 变化的程度 [2] 脑顺应性: Intracranial compliance = Δ P / Δ V 1. Head Injury . Peter Reilly and Ross Bullock. Chapman & Hall, London. 1997; 19. Management of Intracranial Pressure And Cerebral Perfusion. 386 2. John M. Turner. Textbook of neuroanaesthesia and intensive care.52-64 , Greenwich Medical Media LTD, 2000. 经典的颅内压力容积曲线( Monro-Kellie 假说)
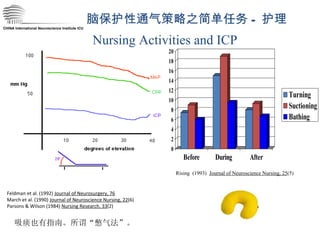
CHINA International NeuroscienceInstitute ICU Feldman et al. (1992) Journal of Neurosurgery, 76 March et al. (1990) Journal of Neuroscience Nursing, 22 (6) Parsons & Wilson (1984) Nursing Research, 33 (2) Nursing Activities and ICP Rising (1993) Journal of Neuroscience Nursing, 25 (5) 脑保护性通气策略之简单任务 - 护理 吸痰也有指南。所谓“憋气法”。
56.
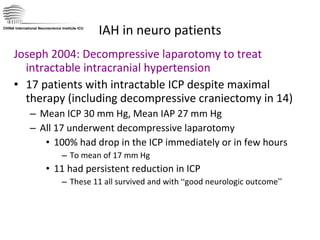
IAH in neuropatients Joseph 2004: Decompressive laparotomy to treat intractable intracranial hypertension 17 patients with intractable ICP despite maximal therapy (including decompressive craniectomy in 14) Mean ICP 30 mm Hg, Mean IAP 27 mm Hg All 17 underwent decompressive laparotomy 100% had drop in the ICP immediately or in few hours To mean of 17 mm Hg 11 had persistent reduction in ICP These 11 all survived and with “ good neurologic outcome ” CHINA International Neuroscience Institute ICU
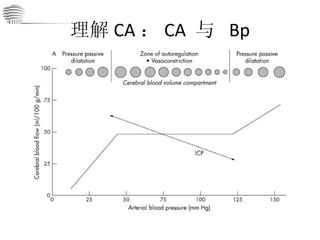
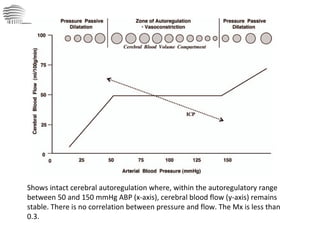
Shows intact cerebralautoregulation where, within the autoregulatory range between 50 and 150 mmHg ABP (x-axis), cerebral blood flow (y-axis) remains stable. There is no correlation between pressure and flow. The Mx is less than 0.3.
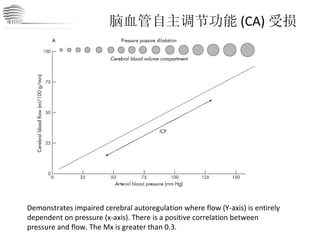
脑血管自主调节功能 (CA) 受损Demonstrates impaired cerebral autoregulation where flow (Y-axis) is entirely dependent on pressure (x-axis). There is a positive correlation between pressure and flow. The Mx is greater than 0.3. CHINA International Neuroscience Institute ICU
69.
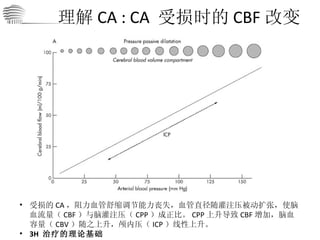
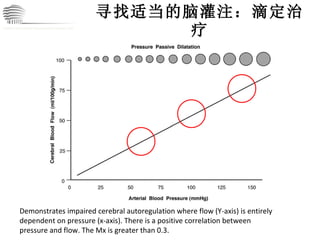
寻找适当的脑灌注:滴定治疗 Demonstrates impairedcerebral autoregulation where flow (Y-axis) is entirely dependent on pressure (x-axis). There is a positive correlation between pressure and flow. The Mx is greater than 0.3. CHINA International Neuroscience Institute ICU
70.
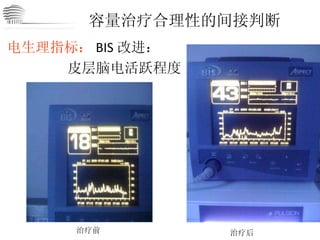
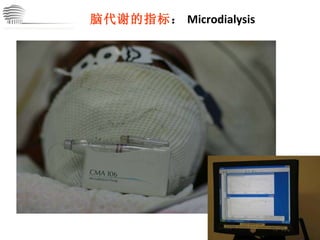
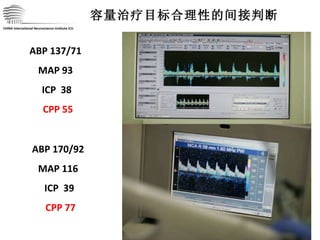
脑灌注滴定治疗合理性的间接判断 压力指标: ICP↓ 和 CPP↑ 容量指标: CO 和 TCD 波形 电生理指标: BIS (脑电双频指数):皮层脑电活跃程度改进 代谢指标: SjVO2 ;神志好转。。。 CHINA International Neuroscience Institute ICU
71.
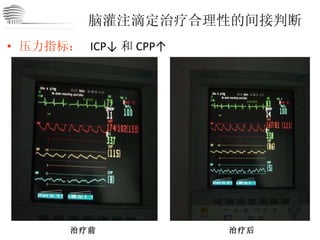
脑灌注滴定治疗合理性的间接判断 压力指标: ICP↓ 和 CPP↑ 治疗前 治疗后 CHINA International Neuroscience Institute ICU
72.
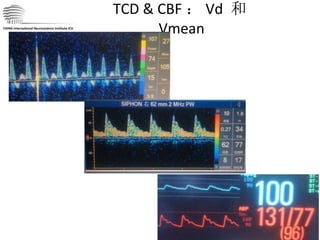
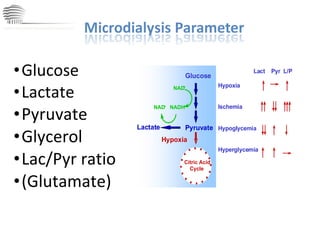
TCD & CBF: Vd 和 Vmean CHINA International Neuroscience Institute ICU
73.
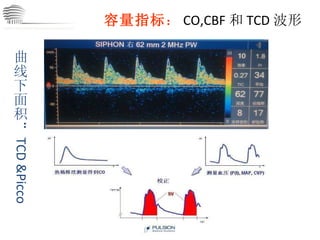
容量指标 : CO,CBF和 TCD 波形 CHINA International Neuroscience Institute ICU 曲线下面积: TCD &Picco
D6 生命体征稳定, ICP已降至 40-50mmHg 明确有自主呼吸,也有自发运动 CHINA International Neuroscience Institute ICU
87.
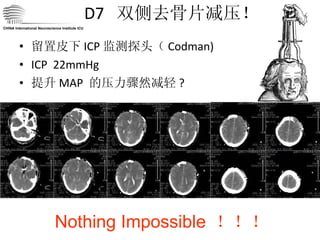
D7 双侧去骨片减压!留置皮下 ICP 监测探头( Codman) ICP 22mmHg 提升 MAP 的压力骤然减轻 ? Nothing Impossible !!! CHINA International Neuroscience Institute ICU
88.
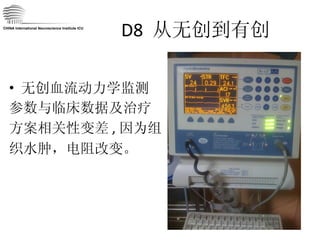
D8 脑血管痉挛但 BIS 逐渐却坚定的降低至 0 :没电了 CHINA International Neuroscience Institute ICU
89.
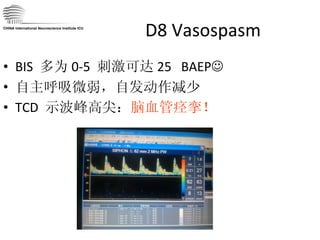
D8 Vasospasm BIS 多为 0-5 刺激可达 25 BAEP 自主呼吸微弱,自发动作减少 TCD 示波峰高尖: 脑血管痉挛! CHINA International Neuroscience Institute ICU
90.
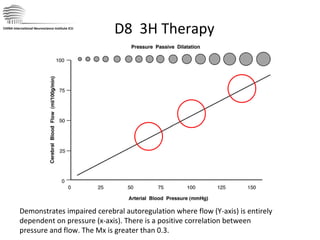
D8 3HTherapy Demonstrates impaired cerebral autoregulation where flow (Y-axis) is entirely dependent on pressure (x-axis). There is a positive correlation between pressure and flow. The Mx is greater than 0.3. CHINA International Neuroscience Institute ICU
91.
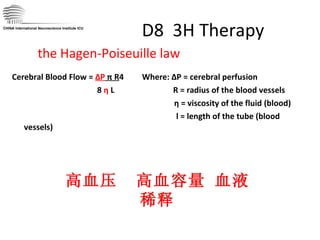
D8 3HTherapy Cerebral Blood Flow = ΔP π R 4 Where: ΔP = cerebral perfusion 8 η L R = radius of the blood vessels η = viscosity of the fluid (blood) l = length of the tube (blood vessels) CHINA International Neuroscience Institute ICU the Hagen-Poiseuille law 高血压 高血容量 血液稀释
92.
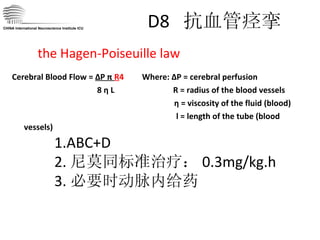
D8 抗血管痉挛Cerebral Blood Flow = ΔP π R 4 Where: ΔP = cerebral perfusion 8 η L R = radius of the blood vessels η = viscosity of the fluid (blood) l = length of the tube (blood vessels) CHINA International Neuroscience Institute ICU the Hagen-Poiseuille law 1.ABC+D 2. 尼莫同标准治疗: 0.3mg/kg.h 3. 必要时动脉内给药
93.
PART 3 小结 CHINA International Neuroscience Institute ICU 不要忘记了我们最初的目的: 不是压力 不是灌注 是 代谢 !!!
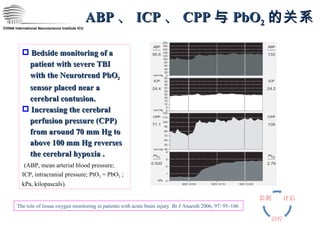
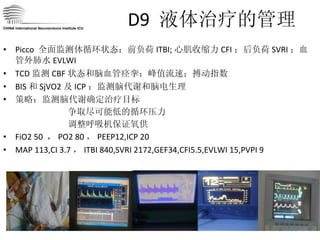
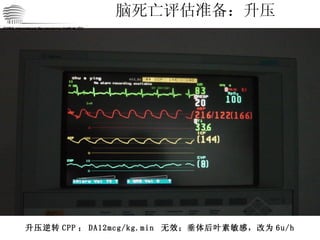
CHINA International NeuroscienceInstitute ICU ABP 、 ICP 、 CPP 与 PbO 2 的关系 Bedside monitoring of a patient with severe TBI with the Neurotrend PbO 2 sensor placed near a cerebral contusion. Increasing the cerebral perfusion pressure (CPP) from around 70 mm Hg to above 100 mm Hg reverses the cerebral hypoxia . (ABP, mean arterial blood pressure; ICP, intracranial pressure; PtO 2 = PbO 2 ; kPa, kilopascals). The role of tissue oxygen monitoring in patients with acute brain injury Br J Anaesth 2006; 97: 95–106
99.
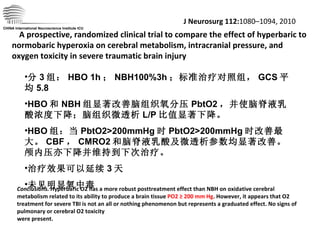
CHINA International NeuroscienceInstitute ICU J Neurosurg 112: 1080–1094, 2010 A prospective, randomized clinical trial to compare the effect of hyperbaric to normobaric hyperoxia on cerebral metabolism, intracranial pressure, and oxygen toxicity in severe traumatic brain injury Conclusions. Hyperbaric O2 has a more robust posttreatment effect than NBH on oxidative cerebral metabolism related to its ability to produce a brain tissue PO2 ≥ 200 mm Hg . However, it appears that O2 treatment for severe TBI is not an all or nothing phenomenon but represents a graduated effect. No signs of pulmonary or cerebral O2 toxicity were present. 分 3 组: HBO 1h ; NBH100%3h ;标准治疗对照组, GCS 平均 5.8 HBO 和 NBH 组显著改善脑组织氧分压 PbtO2 ,并使脑脊液乳酸浓度下降;脑组织微透析 L/P 比值显著下降。 HBO 组:当 PbtO2>200mmHg 时 PbtO2>200mmHg 时改善最大。 CBF , CMRO2 和脑脊液乳酸及微透析参数均显著改善。颅内压亦下降并维持到下次治疗。 治疗效果可以延续 3 天 未见明显氧中毒
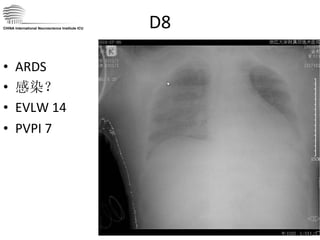
D8 ARDS 感染?EVLW 14 PVPI 7 CHINA International Neuroscience Institute ICU
145.
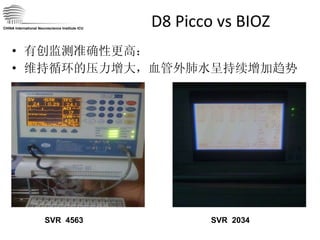
D8 高循环状态和肺水治疗上出现矛盾 ICP 虽较前明显降低, 20-30mmHg (正常 <15 ),但由于脑血管痉挛,有效脑灌注脑电活动下降,支持脑灌注压力仍大,为保证脑循环需要持续高 CO 状态。 但肺水持续增高, ALI ? CHINA International Neuroscience Institute ICU
146.
讨论 4 如何平衡脑灌注和高肺水的矛盾 CHINA International Neuroscience Institute ICU • Is the patient wet or dry? • Do I give volume? • Is there adequate contractility? • Do I give inotropes?
147.
脑保护性通气策略 策略:阶段性允许性肺水肿;寻找最佳 PEEP(脑)和 FiO2 ; HBO ? 治疗目标:阶段性保证氧合,保证高循环状态,保护脑! CHINA International Neuroscience Institute ICU Brain tissure oxygen tesion ---PbtO2
D10 挑战液体分布激素?给了 500 甲强龙 堵漏?堵不上! 白蛋白?给了,高了,肯定也漏了 换抗生素?换就换 CRRT :?血管里没水可拉。虽然正平衡,但有效循环血量不足。 谁能告诉我,如何把水从组织中拉出来?! CHINA International Neuroscience Institute ICU
Startby doing what’s necessary , then do what’s possible , and suddenly you are doing the impossible. —— St . Francis of Assisi 一开始做一些必须做的事情; 接着做有可能的事情; 然后你就会突然发现自己正在做不可能的事情。 —— 圣方济各 Cogito Ergo Sum
170.
我思故我在 我行故我待思考,实践,探索,期待 . . . CHINA International Neuroscience Institute ICU Cogito Ergo Sum
![生命支持与脑灌注 Life support & cerebral perfusion Case Presentation CHINA INI ICU [email_address]](https://image.slidesharecdn.com/random-110821012643-phpapp02/85/slide-1-320.jpg)


![颅内压 ICP 颅腔内容物:神经元,神经胶质细胞,血液,脑脊液,细胞外液 (病理情况下:如内生骨瘤,转移瘤,空气,异物。。。) [1] 任何一项容积发生变化和 / 或出现新的占位(如血肿)等都会使 ICP 发生变化,首发因素的程度和速度等决定了 ICP 变化的程度 [2] 脑顺应性: Intracranial compliance = Δ P / Δ V 1. Head Injury . Peter Reilly and Ross Bullock. Chapman & Hall, London. 1997; 19. Management of Intracranial Pressure And Cerebral Perfusion. 386 2. John M. Turner. Textbook of neuroanaesthesia and intensive care.52-64 , Greenwich Medical Media LTD, 2000. 经典的颅内压力容积曲线( Monro-Kellie 假说)](https://image.slidesharecdn.com/random-110821012643-phpapp02/85/slide-43-320.jpg)
![颅内压 ICP 颅腔内容物:神经元,神经胶质细胞,血液,脑脊液,细胞外液 (病理情况下:如内生骨瘤,转移瘤,空气,异物。。。) [1] 任何一项容积发生变化和 / 或出现新的占位(如血肿)等都会使 ICP 发生变化,首发因素的程度和速度等决定了 ICP 变化的程度 [2] 脑顺应性: Intracranial compliance = Δ P / Δ V 1. Head Injury . Peter Reilly and Ross Bullock. Chapman & Hall, London. 1997; 19. Management of Intracranial Pressure And Cerebral Perfusion. 386 2. John M. Turner. Textbook of neuroanaesthesia and intensive care.52-64 , Greenwich Medical Media LTD, 2000. 经典的颅内压力容积曲线( Monro-Kellie 假说)](https://image.slidesharecdn.com/random-110821012643-phpapp02/85/slide-53-320.jpg)