Traumatic brain injury(TBI) non-TBI 重症患者调查显示:体重丧失 30% 将明显增加患者的病死率 TBI 重症患者蛋白质丢失与体重降低相关,约 15% / week 提供 100 to 140% 的静息能量消耗( RME )及 15 to 20% 蛋白质热卡将获得节氮效应 时机 : 早期营养供给 ( prior to 7 days )能够改善预后 J Neurotrauma 2007;24(Suppl 1):S77
9.
临床营养支持的发展 The past50 years of medicine and critical care have brought great advances in 应激后的代谢与营养改变 营养的合理供给 Optimal carlory Optimal route Right time 营养素与营养支持的治疗作用 Paul E. Wischmeyer, 2010
全面认识营养支持的作用 代谢支持 vs. 营养支持 first week post injury by hypocaloric feedings (50%–75% RME) >1.2 g/kg/d protein as intravenous AA; 应激后肌肉储存 AA 的动员是细胞生存的重要机制 Glucose control 营养支持不是单是营养供给,调节代谢相关的生理状态和改变 Transforming nutrition to a goal-directed therapy
13.
指南涉及的核心问题 时机选择 timing: EN and PN 方式选择: route of nutrition EN: strategies to optimize delivery, risk, intolerance, composition … PN: supply to EN, overfeeding, composition… 目标: dose (energy, nutrients) special composition therapy 实现优化的营养供给和降低风险的策略
14.
Guidelines: 临床操作中掌握的原则(1) General statement 是否存在营养至此的指征: EN 是首先考虑的选择并应在 24 小时开始 争取在如 ICU 3 天左右实现 60% 以上的目标营养供给量 ; 不能达到这应考虑添加肠外途径补充( PN ) Current Opinion in Critical Care 2008, 14:408
15.
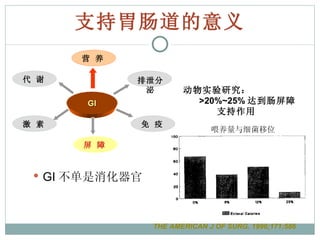
支持胃肠道的意义 GI 不单是消化器官动物实验研究: >20%~25% 达到肠屏障 支持作用 喂养量与细菌移位 THE AMERICAN J OF SURG. 1996;171:586 GI 营 养 排泄分泌 代 谢 屏 障 激 素 免 疫
ADA adequately fluidresuscitated then EN should be started within 24-48 hours following injury or admission to the ICU (A) Canada CPG 2009 update : 基于 14 项 2 级研究结果 , 强力推荐重症病人早期开始肠内营养 ( 入 ICU 24-48 hours) Early vs. Delayed nutrient intake Timing : All guidelines: early EN in critically ill patient Heyland et al, 2009 结论:重症患者 Early EN vs. delayed nutrient intake : 感染性并发症明显降低 病死率降低趋势 LOS 与住 ICU 时间无明显改善 改善了营养摄入
重症病人 EN 早期添加PN 的研究结果: 在改善病死率方面 EN 与 PN 并无差异 无营养不良、消化道完整的重症病人, EN+PN vs. EN only ,对于临床结局改善无有益影响 添加 PN 应在充分尝试增加肠道喂养策略后再与考虑,如:采取小肠喂养、应用肠动力药物 Dhaliwal et al ICM 2004; 30: 1666 CPG 2009 update EN 添加 PN 的指征
21.
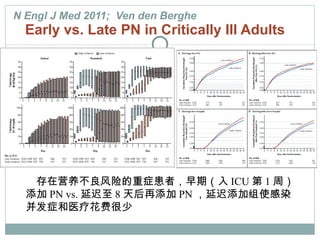
N Engl JMed 2011; Ven den Berghe Early vs. Late PN in Critically Ill Adults 存在营养不良风险的重症患者,早期(入 ICU 第 1 周)添加 PN vs. 延迟至 8 天后再添加 PN ,延迟添加组使感染并发症和医疗花费很少
临床操作中掌握的原则 ( TPN或 EN+PN 的时机) 2007 DGEM-Guideline: 外科 ( C ) 具有营养支持指征 经口或经胃肠道补充量低于需要量的 60% 老年患者应特别关注 Current Opinion in Critical Care 2008, 14:408
24.
临床操作中掌握的原则 三种情况无能使用肠道 severeshock state nonfunctional gut (i.e. anatomic disruption, obstruction, ischemia), severe peritonitis Current Opinion in Critical Care 2008, 14:408
25.
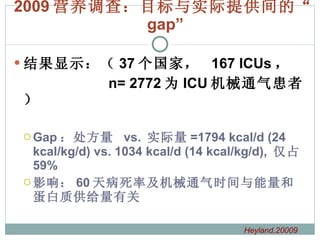
Dose : Therelationship between nutritional intake & outcomes in critically ill pts Results of an international multicenter observational 37 个国家, 167 个 ICU ,队列研究, 12 天营养支持 60-day 病死率与脱离接卸通气时间 (VFDs) BMI, kg/m 2 提示入 ICU 前营养状态 数据来自 2,772 位机械通气,平均接受 1,034 kcal/day and 47 g 蛋白 /day DK. Heyland et al. 2009 ICM; 35
26.
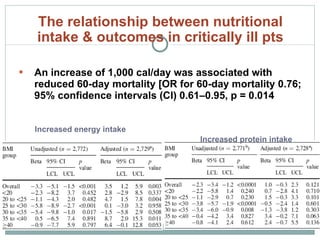
An increase of1,000 cal/day was associated with reduced 60-day mortality [OR for 60-day mortality 0.76; 95% confidence intervals (CI) 0.61–0.95, p = 0.014 Increased energy intake Increased protein intake The relationship between nutritional intake & outcomes in critically ill pts
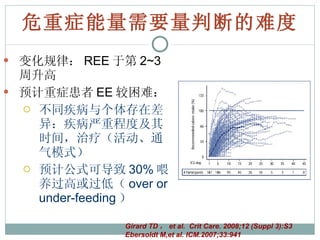
危重症能量需要量判断的难度 变化规律: REE于第 2~3 周升高 预计重症患者 EE 较困难: 不同疾病与个体存在差异:疾病严重程度及其时间,治疗(活动、通气模式) 预计公式可导致 30% 喂养过高或过低( over or under-feeding ) Girard TD , et al. Crit Care. 2008;12 (Suppl 3):S3 Ebersoldt M,et al. ICM.2007;33:941
30.
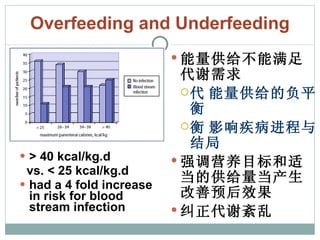
Overfeeding and Underfeeding> 40 kcal/kg.d vs. < 25 kcal/kg.d had a 4 fold increase in risk for blood stream infection 能量供给不能满足代谢需求 能量供给的负平衡 影响疾病进程与结局 强调营养目标和适当的供给量 产生改善预后效果 纠正代谢紊乱
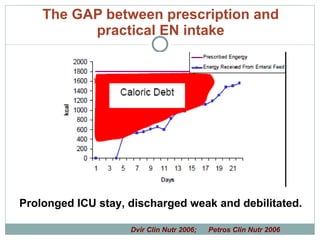
The GAP betweenprescription and practical EN intake Prolonged ICU stay, discharged weak and debilitated. Dvir Clin Nutr 2006; Petros Clin Nutr 2006
34.
神经组织对能量的需求 一项随机对照研究:神经重症患者,第一周供给目标量的能量与氮量 60%~80%(研究组) vs. 30%~50% (对照组): 研究组接受更多的能量供给,和较少的感染性并发症 6 个月神经功能方面的预后指标两组并无差异 颅脑损伤患者早期营养摄入不足与急性相反应延长有关,并增加感染性并发症 糖是脑细胞重要的能源物质 严重颅脑损伤患者脑内微透析测定显示严格血糖控制增加脑细胞能量缺乏和死亡的危险 Taylor SJ , et al. CCM. 1999, 27:2525 Oddo et al. CCM 2008; 36: 3233
35.
神经重症患者营养支持特点 GI 解剖完整功能障碍: 应激性溃疡 GI 动力障碍:胃排空障碍 风险因素: 意识障碍 体位要求 代谢异常:高血糖与低血糖 途径选择特点: PEG :早期( <7d )经胃喂养与返流、肺炎) PEG/J 可能是更安全的选择
36.
An optimal nutritionaltherapy 实施中的考虑 评估 Assessment : 监测 Monitoring :代谢、耐受、并发症 代谢状态 器官功能 根据客观信息才能实现对病情不同的重症病人提供理想的营养治疗 剂量: how many calories should be fed 途径: by what route 营养素: specific nutrients
37.
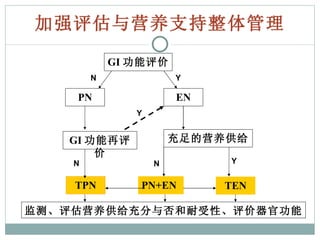
加强评估与营养支持整体管理 GI 功能评价PN PN+EN TPN EN GI 功能再评价 充足的营养供给 TEN Y N Y Y N N 监测、评估营养供给充分与否和耐受性、评价器官功能
38.
营养支持 营养治疗营养支持的地位: not priority, ignore 重症患者营养支持的合理应用: Optimal 规避风险,合理选择 代谢调理,避免和纠正代谢紊乱 对神经细胞的影响: 葡萄糖水平:避免低血糖 蛋白质水平 “ adequate nutrition” 含义 how many calories we provide to provide key pharmacologically acting nutrients.— ‘‘nutritional pharmacology.’’
39.
An optimal nutritionaltherapy 能否从中获益基于对营养支持的整体认识和管理,也基于对患者病情的充分了解,在此基础上作出每位患者最适宜的选择 营养治疗方式( EN or PN )产生的效果在于选择适宜的病人,适宜的时机和恰当的供给量,这样才能使其得到最大获益
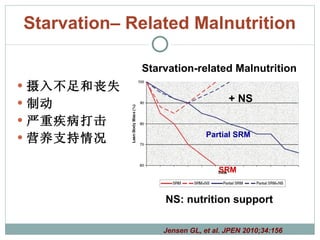
#6 Hypothetical relationship of Starvation-related Malnutrition and Disease-related Malnutrition (bottom graph) assuming the inflammatory condition is relatively constant with changes in lean body mass. For SRM (Red color solid line), Lean body mass is depleted without nutritional intervention but this can be corrected with nutrition support (NS) (SRM+NS, Red color dotted line). During partial SRM (Blue color solid line), lean body mass depletion is slower but still may be reversed by nutrition support (Partial SRM+NS, Blue color dotted line).
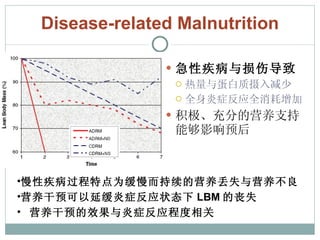
#7 For ADRM (Red color solid line), significant depletion of lean body mass over a short period of time (< 1 month) occurs with no nutritional intervention. With nutritional intervention (Red color dotted line), the loss in lean body mass is abated but loss still occurs if inflammation persists. For CDRM (Blue color dotted line), the loss in lean body mass is gradual and will eventually reach detrimental levels over time (several months). This process could be slowed or potentially reversed with nutritional interventions. In both scenarios, ADRM and CDRM, nutritional intervention may be beneficial but with success dependent on the degree and duration of the inflammatory response. Key: ADRM, acute disease- or injury-related malnutrition; ADRM+NS, ADRM with nutrition support; CDRM, chronic disease-related malnutrition; CDRM+NS, CDRM with nutrition support; SRM, starvation-related malnutrition; SRM+NS, SRM with nutrition support. SRM- starvation-related malnutrition, SRM+NS- starvation-related malnutrition with nutrition support.
#9 Brain Trauma Foundation, American Association of Neurological Surgeons, Congress of Neurological Surgeons,
#10 适宜的时机选择 The treatment of disease with novel pharmacologic agents
#13 potentially new and different therapeutic goal to modulate the systemic inflammatory response might be more effectively accomplished for the first week post injury by hypocaloric feedings (~9–18 kcal/kg or 50%–75% resting metabolic expenditure) principally as intravenous dextrose but with at least 1 g/kg protein as intravenous amino acids to provide early metabolic support
#14 route of nutrition, topics related to EN (use and timing, indirect calorimetry, dose, composition and strategies to optimize delivery and minimize risks, tolerance and other), PN topics (combination parenteral and enteral, parenteral vs standard care, composition, strategies to optimize delivery and minimize risks), and supplemental antioxidants and minerals.
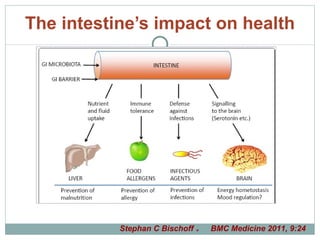
#17 The intestine’s impact on health. The gastrointestinal tract contributes to health by ensuring digestion and absorption of nutrients, minerals and fluids; by induction of mucosal and systemic tolerance; by defence of the host against infectious and other pathogens; and by signalling from the periphery to the brain. For details and references, see text ‘Underlying mechanisms’.
#20 Brain Trauma Foundation, American Association of Neurological Surgeons, Congress of Neurological Surgeons,
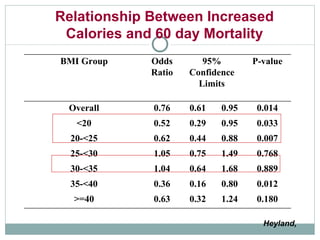
#28 Legend: Odds of 60-day Mortality per 1000 kcals received per day adjusting for nutrition days, BMI, age, admission category, admission diagnosis and APACHE II score.
#37 data-driven care to optimize delivery of nutrition to the diverse population of sick patients Key topics reviewed in this issue include how many calories should be fed and by what route, data for the use of specific nutrients, and finally how to evaluate the plethora of often conflicting nutritional guidelines that exist in critical care.