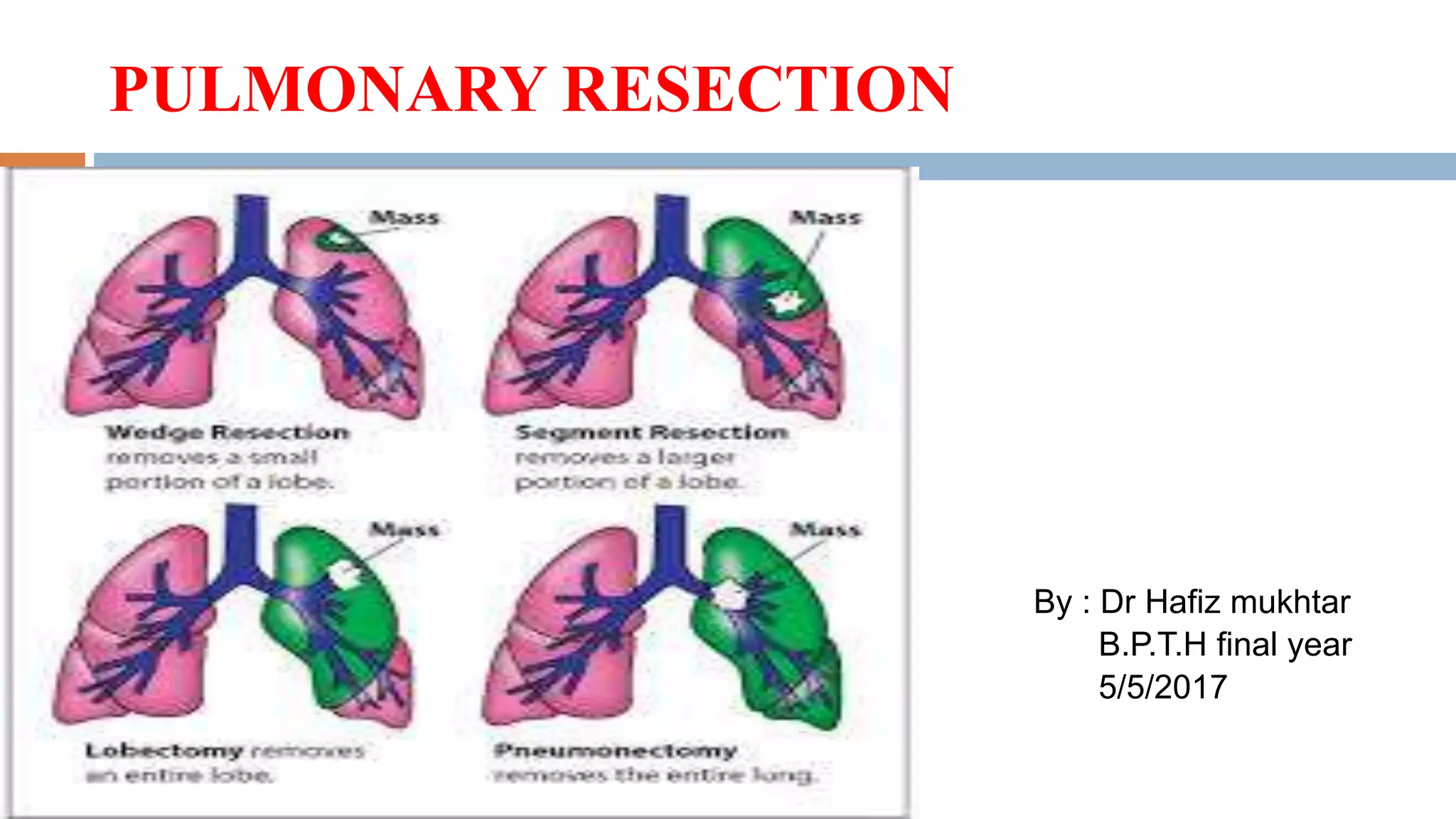
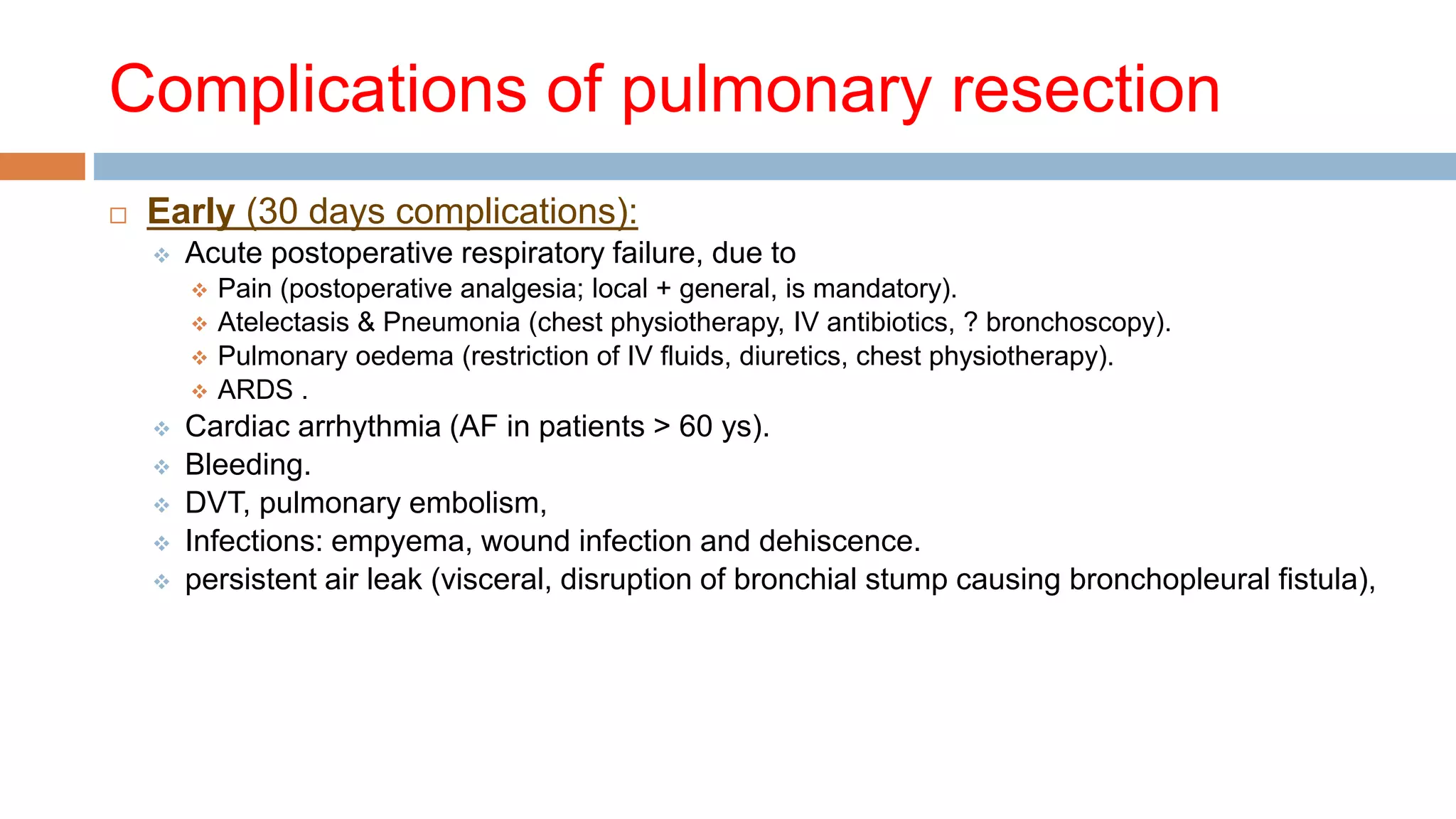
The document discusses pulmonary resection procedures, primarily indicating that bronchial carcinoma is the most common reason for such surgeries. Various types of resections are detailed, including pneumonectomy, lobectomy, segmental resection, and wedge resection, along with their indications and surgical techniques. It also emphasizes the importance of pre-operative and post-operative physiotherapy to enhance recovery and manage complications related to pulmonary resection.














































![Physiotherapy in pulmonary_surgery[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/pulmonarysurgery1-230705093621-2b78f958-thumbnail.jpg?width=640&height=640&fit=bounds)






































