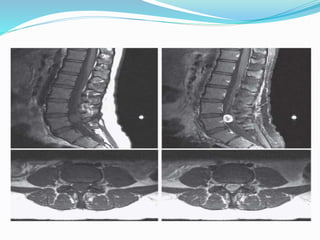
A 25-year-old female presented with a one-year history of lower back pain radiating to both legs. Examination revealed decreased pinprick sensation in the left leg. MRI showed a tumor at L5. The diagnosis was cauda equina syndrome secondary to a spinal meningioma at L5. The patient underwent posterior laminectomy and excision of the tumor. Post-operatively, the patient's pain improved.