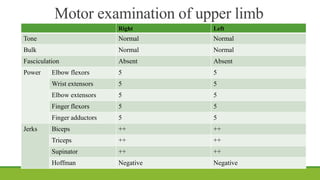
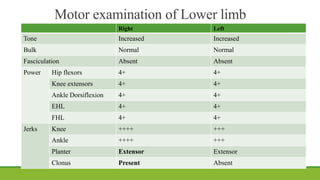
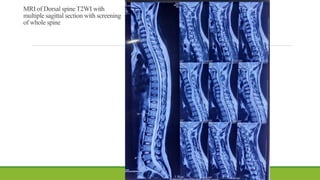
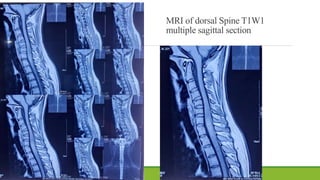
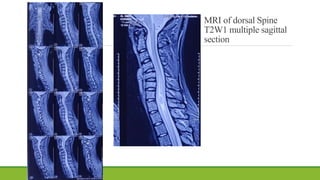
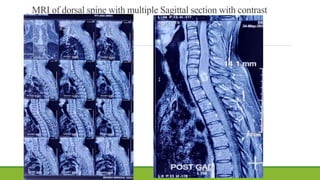
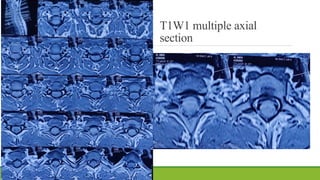
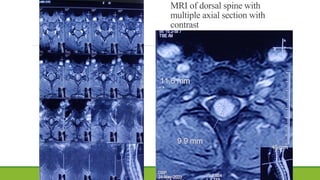
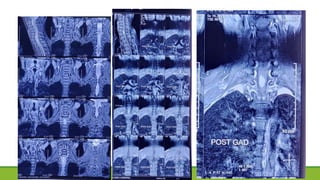
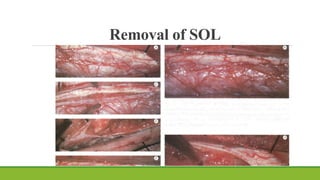
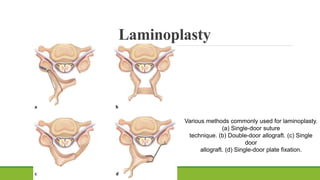
This document presents the case of a 22-year-old male who presented with heaviness in the lower limbs when walking, upper back pain, constipation, and difficulty urinating for 2 months. On examination, he had spastic paraparesis and increased tone, power, and reflexes in the lower limbs. An MRI of the dorsal spine showed an intradural intramedullary lesion from C7 to D1. The clinical and radiological diagnosis was spastic paraparesis due to an intradural intramedullary space-occupying lesion at C7 to D1. The planned treatment was laminotomy and laminoplasty of C7 and D1 with excision of the lesion.