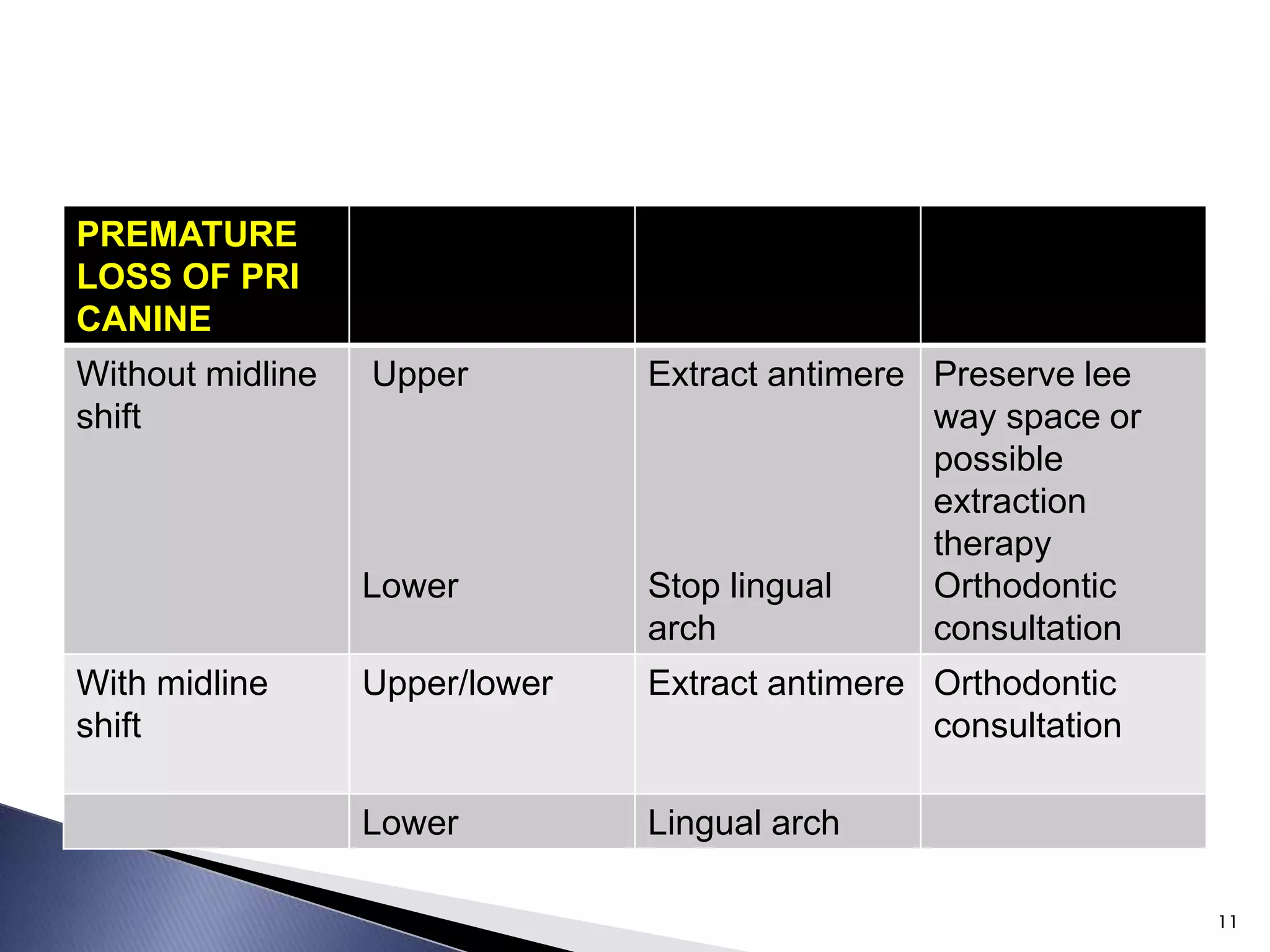
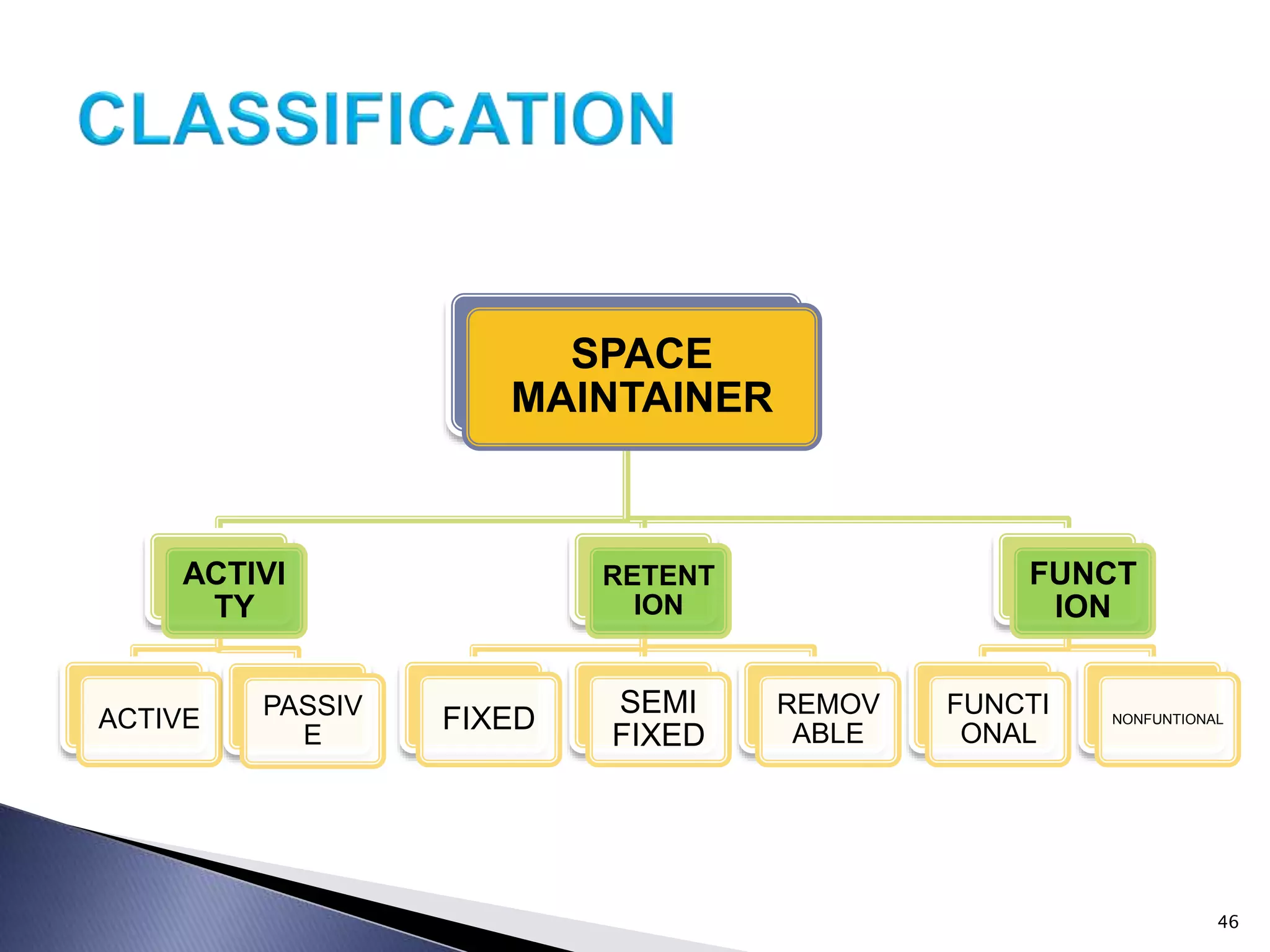
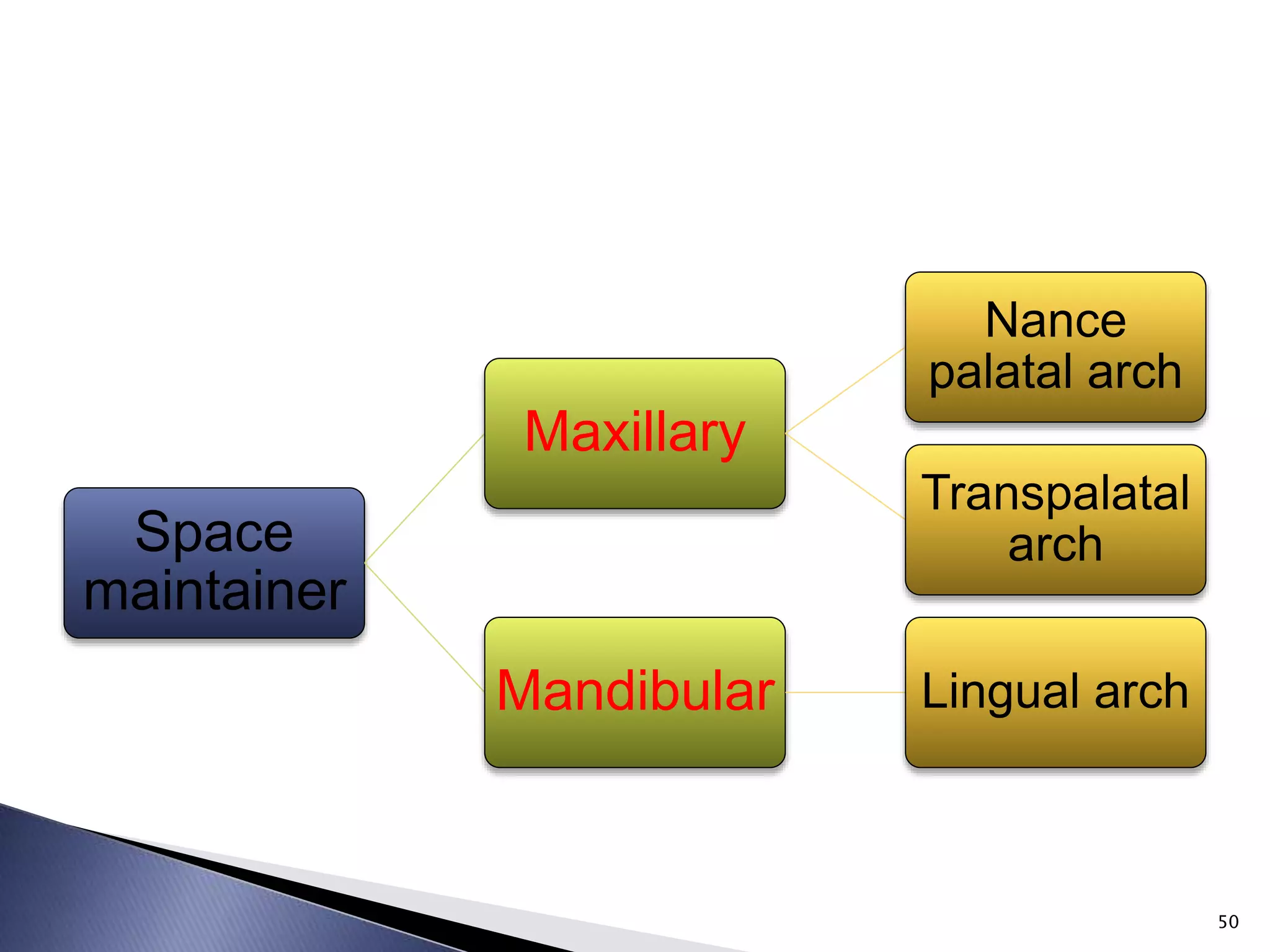
The document discusses preventive orthodontics and space maintenance. It defines preventive orthodontics as actions taken to preserve normal occlusion. Space maintenance involves maintaining space left by premature loss of primary teeth using appliances like bands, lingual arches or removable partial dentures. Factors like dental development stage, eruption timing and bone levels determine need for and type of space maintainer used.
















































































































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)












