Download as PDF, PPTX





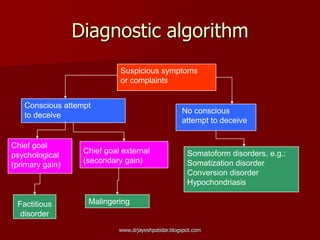





This document discusses somatoform disorders and provides an overview of key topics including: - Definitions and objectives of understanding somatoform disorders - Examples of specific disorders like somatization disorder, hypochondriasis, and conversion disorder - The case of "Ms. A" who has persistent medical complaints and seeks further diagnostic testing - Distinguishing somatoform disorders from conditions like malingering and factitious disorders - Management strategies like explaining the chronic nature of symptoms and exploring their impact on a patient's life
![Somatic Symptom and Related Disorders [2020]](https://cdn.slidesharecdn.com/ss_thumbnails/ssrdv1-200526002841-thumbnail.jpg?width=640&height=640&fit=bounds)


![Somatoform disorders[1]-SEC.A](https://cdn.slidesharecdn.com/ss_thumbnails/somatoformdisorders1-100524061755-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)