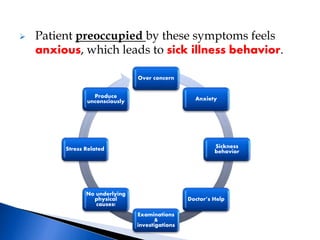
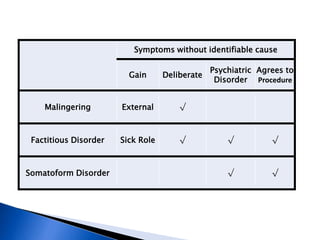
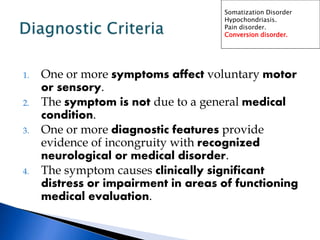
Dr. Ziad N. Arandi discusses somatoform disorders, which are characterized by physical symptoms that cannot be fully explained by medical factors. He outlines four main somatoform disorders - somatization disorder, hypochondriasis, pain disorder, and conversion disorder - providing details on diagnostic criteria and characteristics for each. The treatment approach focuses on supportive psychotherapy, behavioral modification, relaxation therapy, and in some cases antidepressants or benzodiazepines.






![Somatoform disorders[1]-SEC.A](https://cdn.slidesharecdn.com/ss_thumbnails/somatoformdisorders1-100524061755-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)































































