Downloaded 58 times
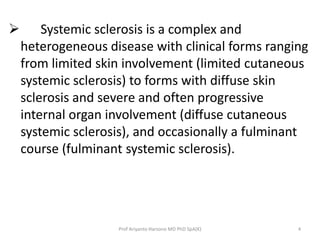

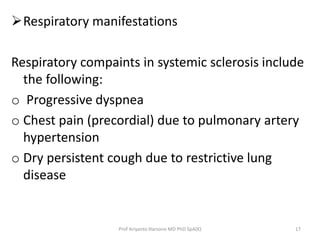

![Atrophy of smooth muscle and submucosal fibrotic changes leading to decreased
peristalsis throughout the gastrointestinal (GI) tract cause gastroesophageal reflux
disease [GERD], gastroparesis, severe constipation, and pseudo-obstruction.
Barium swallow demonstrating reflux into the distal esophagus, as well as an accordion
appearance in the duodenum.
Prof Ariyanto Harsono MD PhD SpA(K) 36](https://image.slidesharecdn.com/sleroderma-141013192410-conversion-gate01/85/Sleroderma-36-320.jpg)

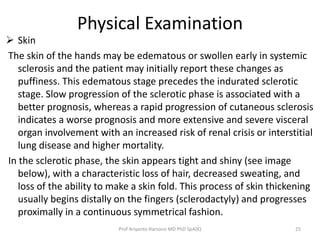
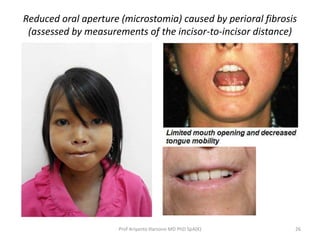
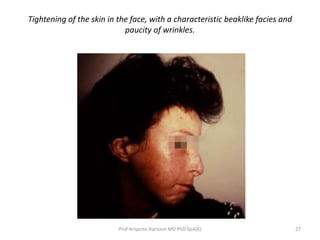
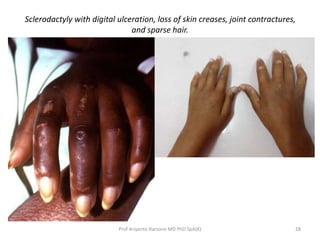
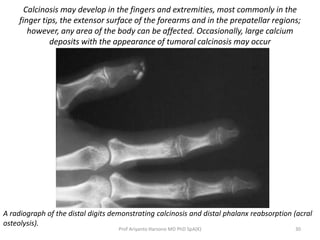
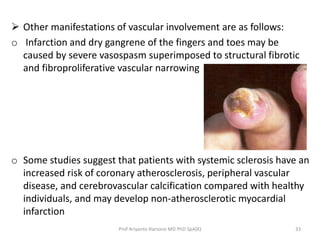
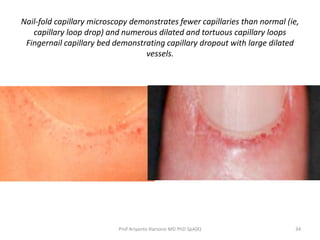
Scleroderma, specifically systemic sclerosis, is a complex autoimmune disease characterized by skin hardening and collagen deposition affecting various organs. It has limited and diffuse forms, with varied clinical manifestations including skin tightness, pulmonary hypertension, and gastrointestinal issues. The disease's pathogenesis involves immune dysfunction, collagen deposition, and environmental factors, contributing to its high morbidity and mortality rates.











































































































