Downloaded 522 times

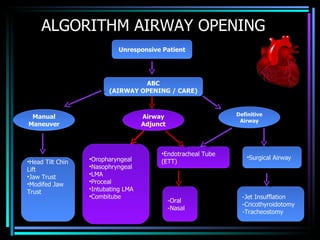
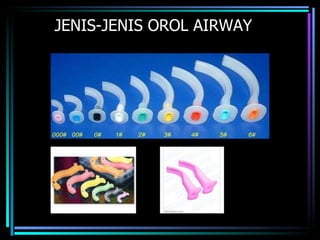
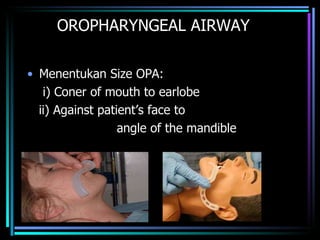
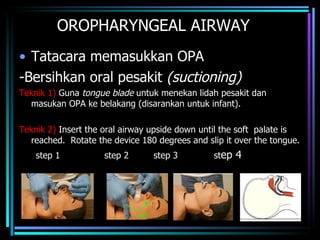
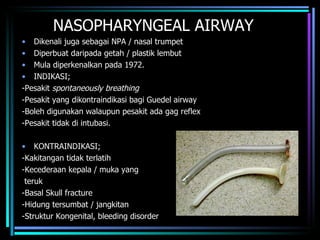
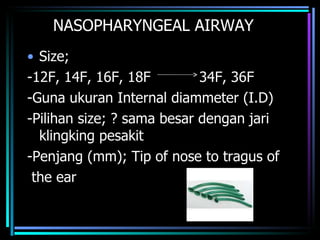
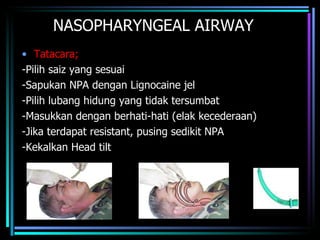
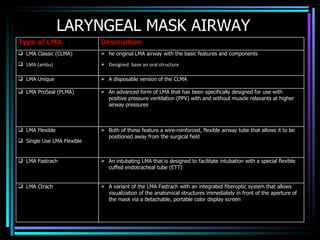
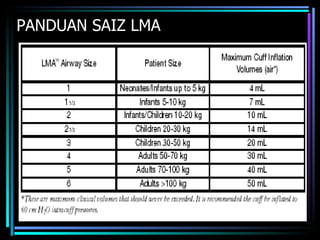
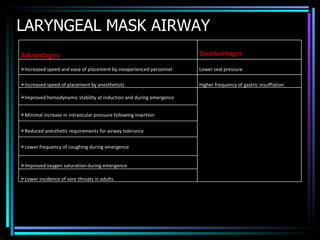
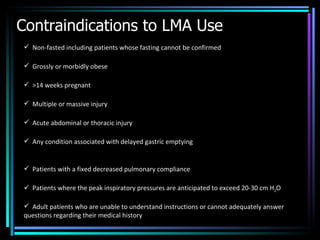
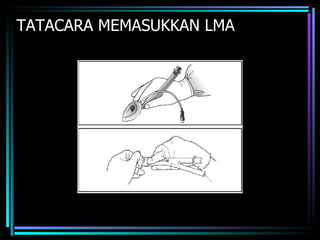
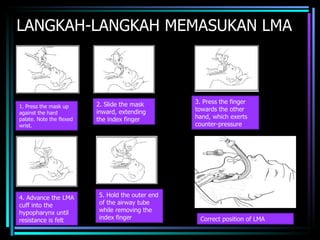

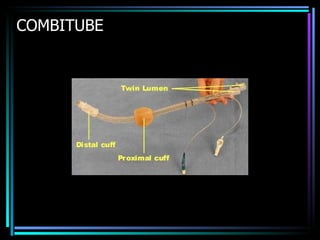
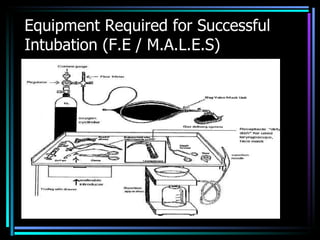
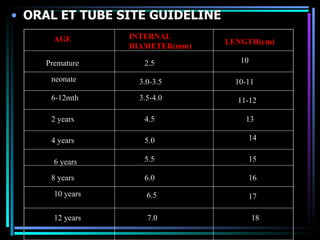
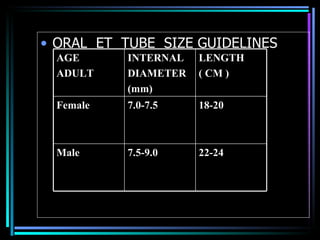
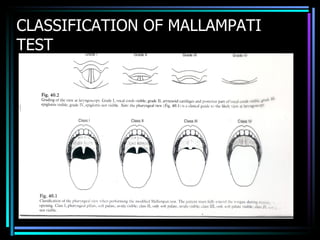
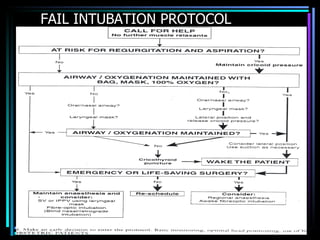
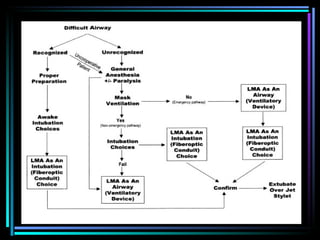

The document discusses various airway management devices and techniques used in basic life support. It describes oropharyngeal airways, nasopharyngeal airways, laryngeal mask airways, endotracheal tubes, and difficult airway management devices like the Combitube. Guidelines for sizing and inserting these devices are provided, along with their indications, contraindications, and potential complications. Factors that can make intubation difficult are also outlined.























































































