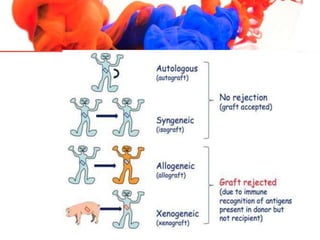
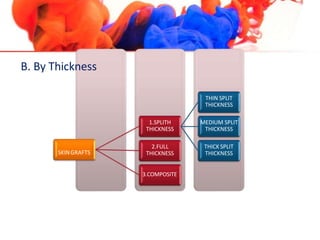
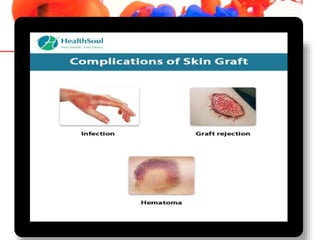
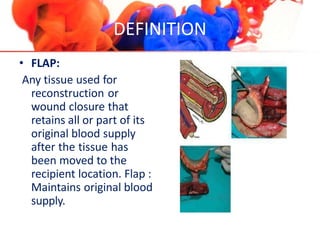
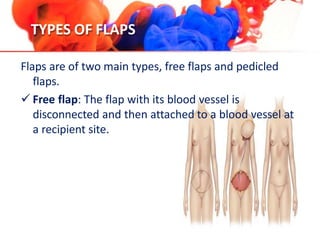
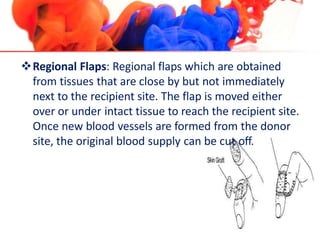
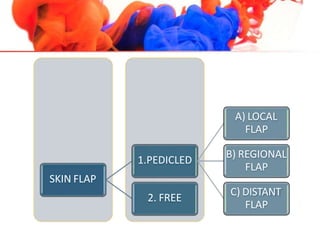
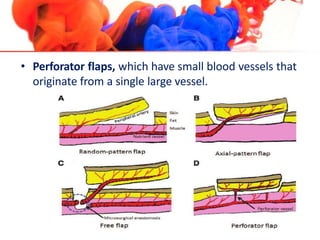
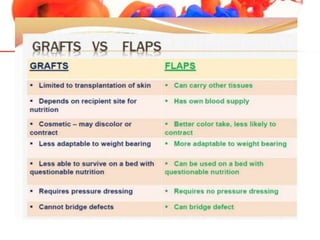
Skin grafting and skin flaps are surgical procedures used to repair skin defects and promote wound healing. In skin grafting, healthy skin is removed from a donor site and transplanted to the recipient site, but does not maintain its original blood supply. Skin flaps involve moving a piece of skin with an intact blood supply from a donor site to the recipient site. There are several types of grafts and flaps classified by thickness, species, or how they obtain their blood supply. Care of the graft/flap and donor site is important for proper healing. Complications can include infection, necrosis, or loss of the graft/flap if blood supply is compromised.













































![Reconstructive and cosmetic surgeries [Auto-saved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/reconstructiveandcosmeticsurgeriesauto-saved-230621074305-25a142e9-thumbnail.jpg?width=640&height=640&fit=bounds)



















































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)


